Bone-Preserving Decompression Procedures Have a Minor Effect on the Flexibility of the Lumbar Spine
- Affiliations
-
- 1Department of Neurosurgery, Humanitas Clinical and Research Center, Rozzano, Italy.
- 2LaBS, Department of Chemistry, Material and Chemical Engineering, Politecnico di Milano, Milano, Italy.
- 3Institute of Orthopaedic Research and Biomechanics, Trauma Research Centre Ulm, Ulm University, Ulm, Germany.
- 4IRCCS Galeazzi Orthopedic Institute, Milano, Italy. fabio.galbusera@grupposandonato.it
- KMID: 2428109
- DOI: http://doi.org/10.3340/jkns.2018.0023
Abstract
OBJECTIVE
To mitigate the risk of iatrogenic instability, new posterior decompression techniques able to preserve musculoskeletal structures have been introduced but never extensively investigated from a biomechanical point of view. This study was aimed to investigate the impact on spinal flexibility caused by a unilateral laminotomy for bilateral decompression, in comparison to the intact condition and a laminectomy with preservation of a bony bridge at the vertebral arch. Secondary aims were to investigate the biomechanical effects of two-level decompression and the quantification of the restoration of stability after posterior fixation.
METHODS
A universal spine tester was used to measure the flexibility of six L2-L5 human spine specimens in intact conditions and after decompression and fixation surgeries. An incremental damage protocol was applied : 1) unilateral laminotomy for bilateral decompression at L3-L4; 2) on three specimens, the unilateral laminotomy was extended to L4-L5; 3) laminectomy with preservation of a bony bridge at the vertebral arch (at L3-L4 in the first three specimens and at L4-L5 in the rest); and 4) pedicle screw fixation at the involved levels.
RESULTS
Unilateral laminotomy for bilateral decompression had a minor influence on the lumbar flexibility. In flexion-extension, the median range of motion increased by 8%. The bone-preserving laminectomy did not cause major changes in spinal flexibility. Two-level decompression approximately induced a twofold destabilization compared to the single-level treatment, with greater effect on the lower level. Posterior fixation reduced the flexibility to values lower than in the intact conditions in all cases.
CONCLUSION
In vitro testing of human lumbar specimens revealed that unilateral laminotomy for bilateral decompression and bone-preserving laminectomy induced a minor destabilization at the operated level. In absence of other pathological factors (e.g., clinical instability, spondylolisthesis), both techniques appear to be safe from a biomechanical point of view.
Keyword
MeSH Terms
Figure
-
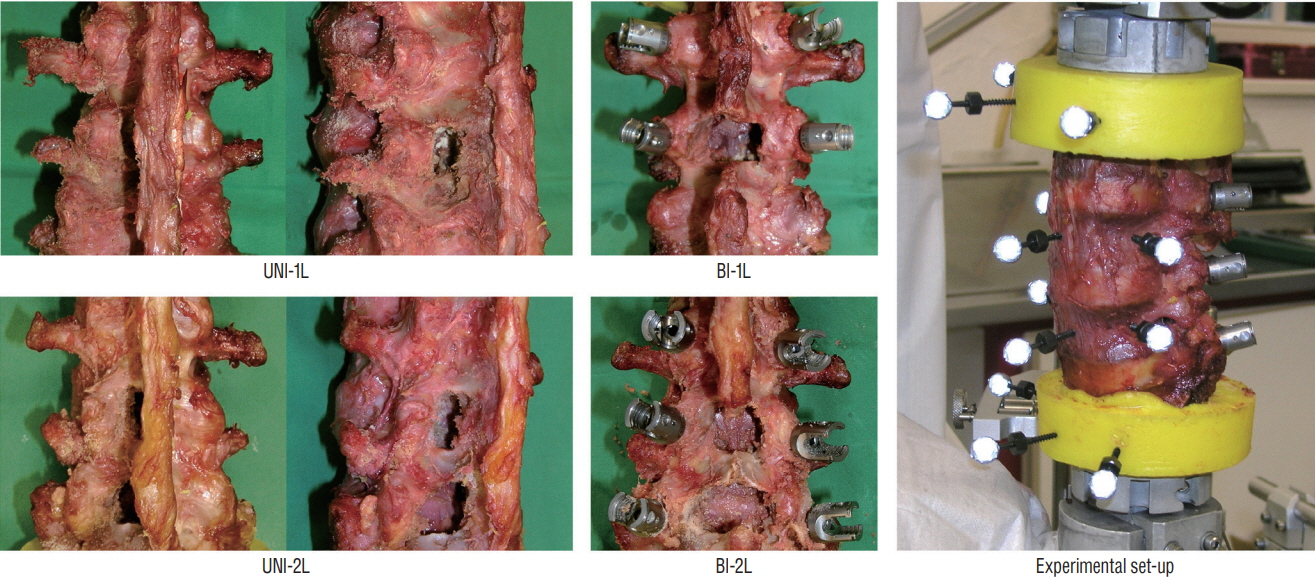
Fig. 1. Decompression and stabilization procedures performed on the specimens : unilateral laminotomy for bilateral decompression at L3–L4 (UNI-1L, n=6 specimens); bone-preserving laminectomy at L3–L4 (BI-1L, n=3); unilateral laminotomy for bilateral decompression at L3–L5 (UNI-2L, n=3); bonepreserving laminectomy at L3–L5 (BI-2L, n=3). Experimental set-up used for load application and motion analysis with an optoelectronic motion analysis system (right).
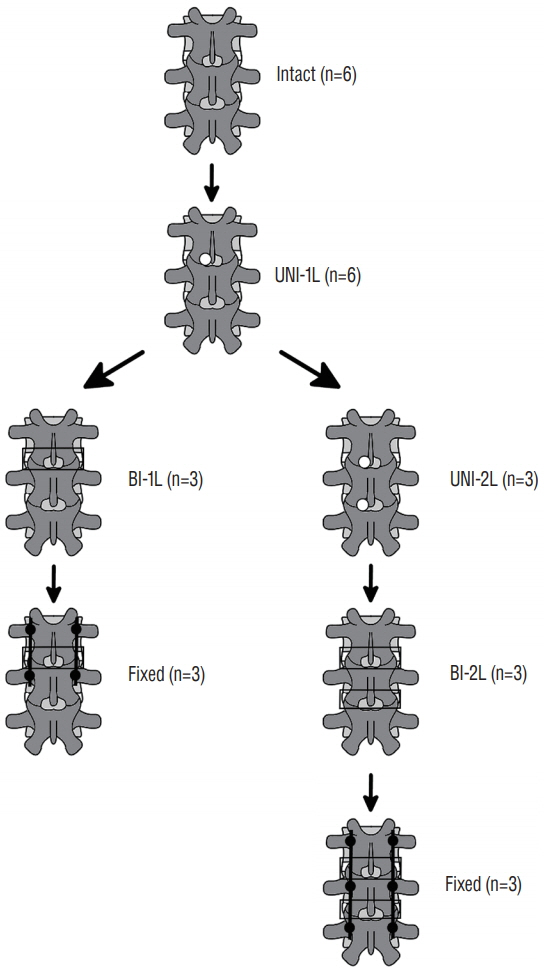
Fig. 2. Schematic representation of the incremental protocol of decompression and fixation. Intact : specimens before decompression, UNI-1L : after unilateral laminotomy for bilateral decompression at L3–L4, UNI-2L : after unilateral laminotomy for bilateral decompression at L3–L5, BI-1L : after bone-preserving laminectomy at L3–L4, BI-2L : after bone-preserving laminectomy at L3–L5, fixed : after posterior fixation with pedicle screws and titanium rods at L3–L4 or L3–L5.

Fig. 3. Photographs (top) and anteroposterior radiographic projections (bottom) of specimens after bone-preserving laminectomy at L3–L4 (left) and L3–L5 (right).
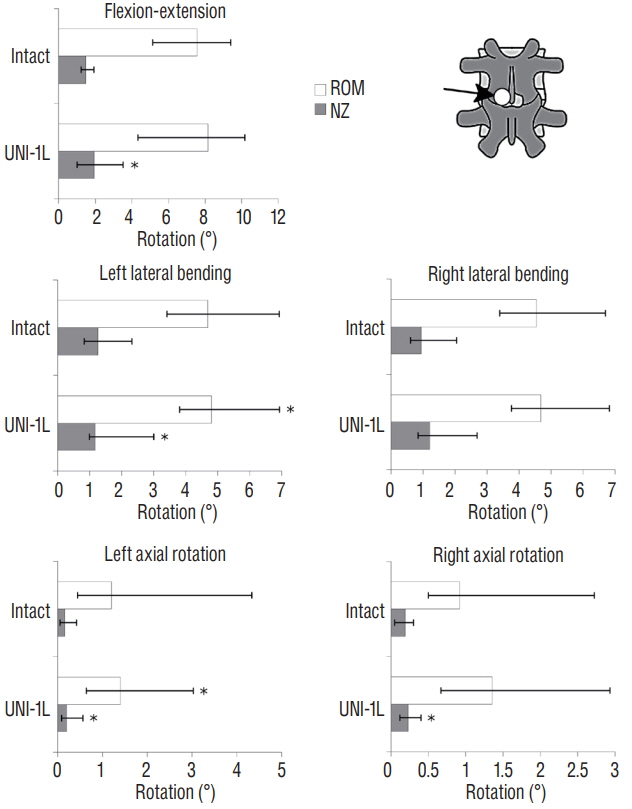
Fig. 4. Statistical comparison of the range of motion (ROM) and neutral zone (NZ) between the intact specimens and those subjected to unilateral laminotomy for bilateral decompression at L3–L4 (UNI-1L), in fiexionextension, left and right lateral bending, left and right axial rotation. *A statistically significant difference (p<0.05) between the intact and the decompressed condition (n=6).
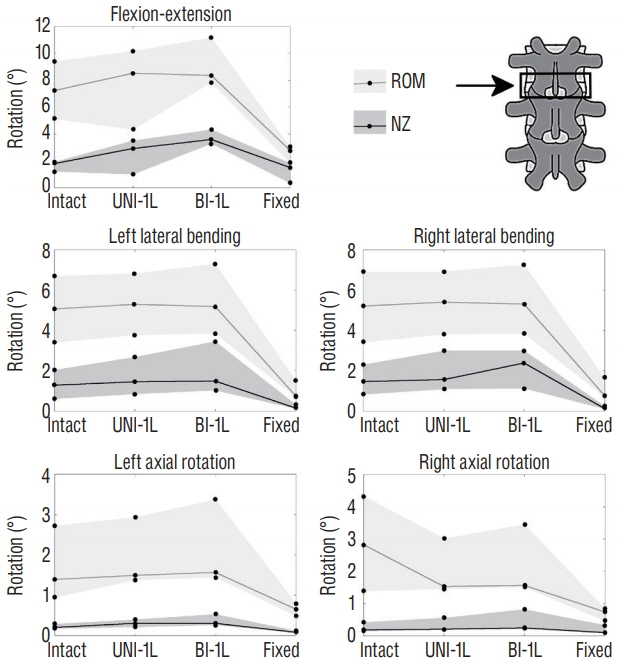
Fig. 5. Changes in the range of motion (ROM) and neutral zone (NZ) of the L3–L4 motion segment (indicated by the arrow) due to incremental decompression performed at the same level, in flexion-extension, left and right lateral bending, left and right axial rotation. The gray areas indicate the range between the maximum and minimum ROM and NZ among the three specimens, whereas the solid lines indicate the median value. Intact : specimen before decompression, UNI-1L : after unilateral laminotomy for bilateral decompression at L3–L4, BI-1L : after bone-preserving laminectomy at L3–L4, fixed : after posterior fixation with pedicle screws and titanium rods at L3–L4.
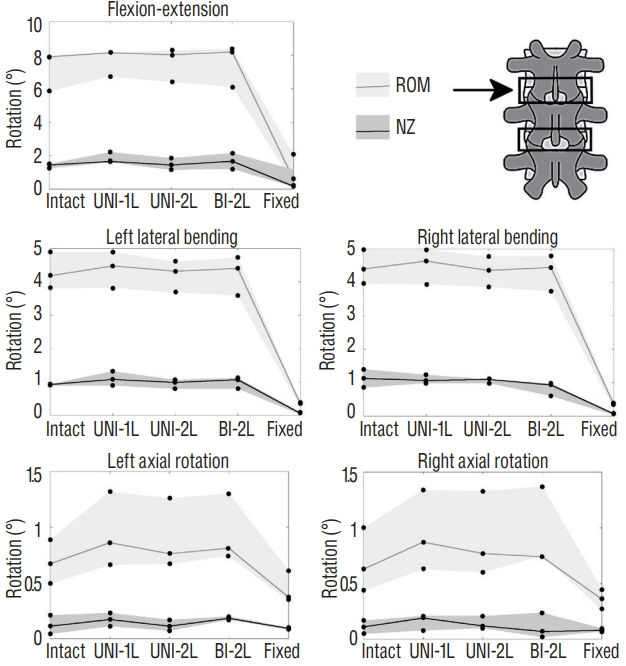
Fig. 6. Changes in the range of motion (ROM) and neutral zone (NZ) of the L3–L4 motion segment (indicated by the arrow) due to incremental decompression performed at the L3–L4 and L4–L5, in fiexion-extension, left and right lateral bending, left and right axial rotation. The gray areas indicate the range between the maximum and minimum ROM and NZ among the three specimens, whereas the solid lines indicate the median value. Intact : specimen before decompression, UNI-1L : after unilateral laminotomy for bilateral decompression at L3–L4, UNI-2L : after unilateral laminotomy at L3–L5, BI-1L : after bone-preserving laminectomy at L3–L5, fixed : after posterior fixation with pedicle screws and titanium rods at L3–L5.
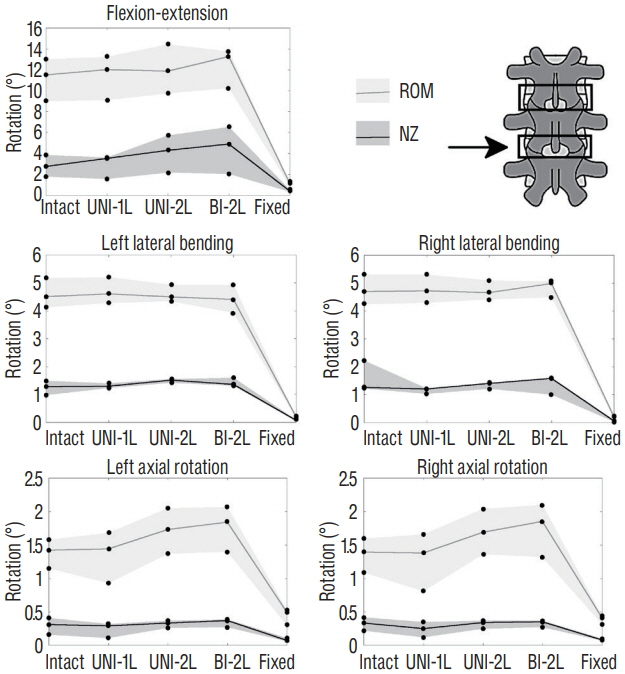
Fig. 7. Changes in the range of motion (ROM) and neutral zone (NZ) of the L4–L5 motion segment (indicated by the arrow) due to incremental decompression performed at the L3–L4 and L4–L5, in fiexion-extension, left and right lateral bending, left and right axial rotation. The gray areas indicate the range between the maximum and minimum ROM and NZ among the three specimens, whereas the solid lines indicate the median value. Intact : specimen before decompression, UNI-1L : after unilateral laminotomy for bilateral decompression at L3–L4, UNI-2L : after unilateral laminotomy at L3–L5, BI-1L : after bone-preserving laminectomy at L3–L5, fixed : after posterior fixation with pedicle screws and titanium rods at L3–L5.
Reference
-
References
1. Airaksinen O, Herno A, Turunen V, Saari T, Suomlainen O. Surgical outcome of 438 patients treated surgically for lumbar spinal stenosis. Spine (Phila Pa 1976). 22:2278–2282. 1997.
Article2. Allen BL Jr, Tencer AF, Ferguson RL. The biomechanics of decompressive laminectomy. Spine (Phila Pa 1976). 12:803–808. 1987.
Article3. Bisschop A, Kingma I, Bleys RL, van der Veen AJ, Paul CP, van Dieën JH, et al. Which factors prognosticate rotational instability following lumbar laminectomy? Eur Spine J. 22:2897–2903. 2013.
Article4. Bisschop A, van Engelen SJ, Kingma I, Holewijn RM, Stadhouder A, van der Veen AJ, et al. Single level lumbar laminectomy alters segmental biomechanical behavior without affecting adjacent segments. Clin Biomech (Bristol, Avon). 29:912–917. 2014.
Article5. Bisschop A, van Royen BJ, Mullender MG, Paul CP, Kingma I, Jiya TU, et al. Which factors prognosticate spinal instability following lumbar laminectomy? Eur Spine J. 21:2640–2648. 2012.
Article6. Carreon LY, Puno RM, Dimar JR 2nd, Glassman SD, Johnson JR. Perioperative complications of posterior lumbar decompression and arthrodesis in older adults. J Bone Joint Surg Am. 85-A:2089–2092. 2003.
Article7. Costa F, Sassi M, Cardia A, Ortolina A, De Santis A, Luccarelli G, et al. Degenerative lumbar spinal stenosis: analysis of results in a series of 374 patients treated with unilateral laminotomy for bilateral microdecompression. J Neurosurg Spine. 7:579–586. 2007.
Article8. diPierro CG, Helm GA, Shaffrey CI, Chadduck JB, Henson SL, Malik JM, et al. Treatment of lumbar spinal stenosis by extensive unilateral decompression and contralateral autologous bone fusion: operative technique and results. J Neurosurg. 84:166–173. 1996.
Article9. Fox MW, Onofrio BM, Hanssen AD. Clinical outcomes and radiological instability following decompressive lumbar laminectomy for degenerative spinal stenosis: a comparison of patients undergoing concomitant arthrodesis versus decompression alone. J Neurosurg. 85:793–802. 1996.
Article10. Fritz JM, Erhard RE, Vignovic M. A nonsurgical treatment approach for patients with lumbar spinal stenosis. Phys Ther. 77:962–973. 1997.
Article11. Fujita T, Kostuik JP, Huckell CB, Sieber AN. Complications of spinal fusion in adult patients more than 60 years of age. Orthop Clin North Am. 29:669–678. 1998.
Article12. Grob D, Humke T, Dvorak J. Degenerative lumbar spinal stenosis. Decompression with and without arthrodesis. J Bone Joint Surg Am. 77:1036–1041. 1995.
Article13. Iguchi T, Kurihara A, Nakayama J, Sato K, Kurosaka M, Yamasaki K. Minimum 10-year outcome of decompressive laminectomy for degenerative lumbar spinal stenosis. Spine (Phila Pa 1976). 25:1754–1759. 2000.
Article14. Ivanov A, Faizan A, Sairyo K, Ebraheim N, Biyani A, Goel VK. Minimally invasive decompression for lumbar spinal canal stenosis in younger age patients could lead to higher stresses in the remaining neural arch -- a finite element investigation. Minim Invasive Neurosurg. 50:18–22. 2007.
Article15. Kato Y, Panjabi MM, Nibu K. Biomechanical study of lumbar spinal stability after osteoplastic laminectomy. J Spinal Disord. 11:146–150. 1998.
Article16. Katz JN, Lipson SJ, Larson MG, McInnes JM, Fossel AH, Liang MH. The outcome of decompressive laminectomy for degenerative lumbar stenosis. J Bone Joint Surg Am. 73:809–816. 1991.
Article17. Kirkaldy-Willis WH, Farfan HF. Instability of the lumbar spine. Clin Orthop Relat Res. 165:110–123. 1982.
Article18. Nakai O, Ookawa A, Yamaura I. Long-term roentgenographic and functional changes in patients who were treated with wide fenestration for central lumbar stenosis. J Bone Joint Surg Am. 73:1184–1191. 1991.
Article19. Phillips FM, Tzermiadianos MN, Voronov LI, Havey RM, Carandang G, Renner SM, et al. Effect of the total facet arthroplasty system after complete laminectomy-facetectomy on the biomechanics of implanted and adjacent segments. Spine J. 9:96–102. 2009.
Article20. Pope MH, Panjabi M. Biomechanical definitions of spinal instability. Spine (Phila Pa 1976). 10:255–256. 1985.
Article21. Quint U, Wilke HJ, Löer F, Claes L. Laminectomy and functional impairment of the lumbar spine: the importance of muscle forces in flexible and rigid instrumented stabilization--a biomechanical study in vitro. Eur Spine J. 7:229–238. 1998.
Article22. Silvers HR, Lewis PJ, Asch HL. Decompressive lumbar laminectomy for spinal stenosis. J Neurosurg. 78:695–701. 1993.
Article23. Simotas AC, Dorey FJ, Hansraj KK, Cammisa F Jr. Nonoperative treatment for lumbar spinal stenosis. clinical and outcome results and a 3-year survivorship analysis. Spine (Phila Pa 1976). 25:197–203. 2000.24. Tanaka N, An HS, Lim TH, Fujiwara A, Jeon CH, Haughton VM. The relationship between disc degeneration and flexibility of the lumbar spine. Spine J. 1:47–56. 2001.
Article25. Thomé C, Zevgaridis D, Leheta O, Bäzner H, Pöckler-Schöniger C, Wöhrle J, et al. Outcome after less-invasive decompression of lumbar spinal stenosis: a randomized comparison of unilateral laminotomy, bilateral laminotomy, and laminectomy. J Neurosurg Spine. 3:129–141. 2005.
Article26. Tuite GF, Stern JD, Doran SE, Papadopoulos SM, McGillicuddy JE, Oyedijo DI, et al. Outcome after laminectomy for lumbar spinal stenosis. Part I: clinical correlations. J Neurosurg. 81:699–706. 1994.27. Verbiest H. A radicular syndrome from developmental narrowing of the lumbar vertebral canal. J Bone Joint Surg Br. 36-B:230–237. 1954.
Article28. Volkheimer D, Malakoutian M, Oxland TR, Wilke WJ. Limitations of current in vitro test protocols for investigation of instrumented adjacent segment biomechanics: critical analysis of the literature. Eur Spine J. 24:1882–1892. 2015.
Article29. White AA, Panjabi MM. Clinical biomechanics of the spine. ed 2. Philadelphia: Lippincott Williams & Wilkins;1990.30. Wilke HJ, Claes L, Schmitt H, Wolf S. A universal spine tester for in vitro experiments with muscle force simulation. Eur Spine J. 3:91–97. 1994.
Article31. Wilke HJ, Wenger K, Claes L. Testing criteria for spinal implants: recommendations for the standardization of in vitro stability testing of spinal implants. Eur Spine J. 7:148–154. 1998.
Article32. Zander T, Rohlmann A, Klöckner C, Bergmann G. Influence of graded facetectomy and laminectomy on spinal biomechanics. Eur Spine J. 12:427–434. 2003.
Article33. Zhao F, Pollintine P, Hole BD, Dolan P, Adams MA. Discogenic origins of spinal instability. Spine (Phila Pa 1976). 30:2621–2630. 2005.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Indirect decompression as a minimally invasive spine surgery
- Nonlaminotomy bilateral decompression: a novel approach in biportal endoscopic spine surgery for spinal stenosis
- Treatment Concept and Technical Considerations of Biportal Endoscopic Spine Surgery for Lumbar Spinal Stenosis
- Evolution of Percutaneous Endoscopic Lumbar Decompression
- The Efficacy of Proximal Lumbar Curve Flexibility in Patients with Main Thoracic Adolescent Idiopathic Scoliosis Treated by Selective Thoracic Fusion Surgery
