Practical Guidelines for Ultrasound-Guided Core Needle Biopsy of Soft-Tissue Lesions: Transformation from Beginner to Specialist
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea. chung@amc.seoul.kr
- 2Department of Radiology, Dankook University Hospital, Cheonan 31116, Korea.
- 3Department of Orthopedic Surgery, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea.
- KMID: 2427948
- DOI: http://doi.org/10.3348/kjr.2017.18.2.361
Abstract
- Ultrasound-guided core needle biopsy (US-CNB) is an important step in the diagnosis of musculoskeletal soft-tissue lesions. To maximize efficacy and minimize the complications of US-CNB, it is critical to collaborate with a multidisciplinary team and to understand the particular considerations of US-CNB for these lesions. The purpose of this article is to provide a systematic review and step-by-step tips for using US-CNB to diagnose musculoskeletal soft-tissue lesions.
MeSH Terms
Figure
-
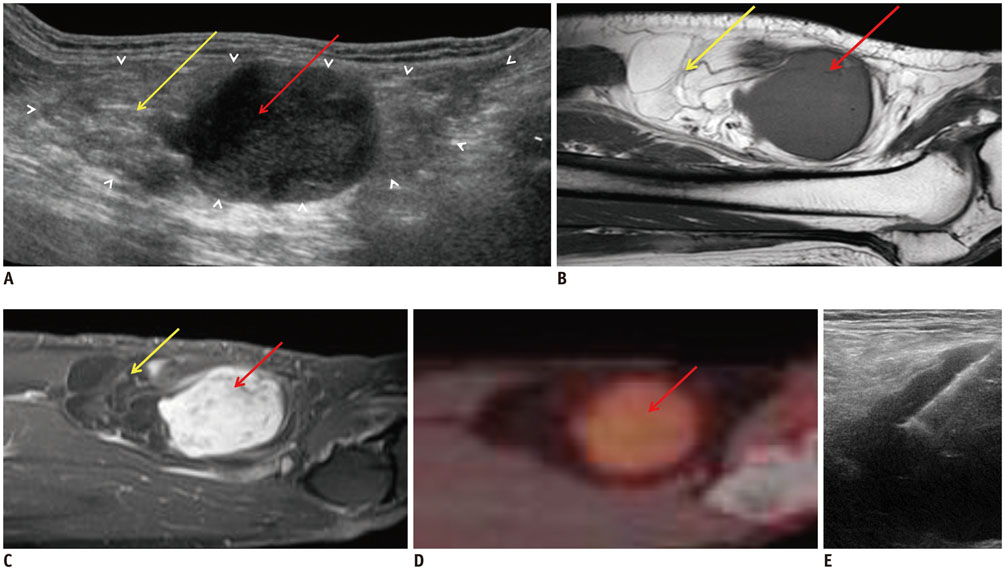
Fig. 1 67-year-old female patient with mass in her right posterior thigh. A. Longitudinal US image showing mass with well-defined, ovoid margins (white arrowheads). Proximal portion of mass (yellow arrow) shows heterogeneous hyper-echogenicity, and distal portion (red arrow) shows homogeneous hypoechogenicity. Deciding proper target is deliberate process for successful US-CNB. B-D. Sagittal T1-weighted MR image (B), enhanced T1-weighted MR image (C), and positron emission tomography (PET) image (D). Proximal portion of mass (yellow arrows) shows high signal intensity with multiple septations on sagittal T1-weighted MR image. This portion does not demonstrate enhancement on enhanced T1-weighted image, thus suggesting fat component. In contrast, distal portion (red arrows) shows homogeneous, intense enhancement on enhanced T1-weighted image and hypermetabolic activity on PET image. When we consider proper targeting, distal portion (red arrow) is best. E. On longitudinal US image, US-CNB was performed at distal hypoechoic area, and this mass was confirmed as well-differentiated liposarcoma. US = ultrasonography, US-CNB = ultrasound-guided core needle biopsy

Fig. 2 55-year-old female patient with mass in her right anterior thigh. A. Longitudinal US image shows multi-lobulated mass. Most proximal portion of mass (red arrow) shows homogeneous hypoechogenicity, and just distal portion (yellow arrow) shows heterogeneous hyperechogenecity; lower portion (white arrow) shows homogeneous hyperechogenecity. It was difficult to determine proper target by considering only ultrasonographic appearance. B, C. On sagittal enhanced T1-weighted MR (B) and PET images (C), most proximal portion of mass (red arrows) enhanced well and revealed hypermetabolic activity. Just distal portion (yellow arrows) shows mild enhancement on enhanced T1-weighted image; however, this portion does not show significant metabolic activity on PET image. Lower portion (white arrows) reveals nonenhancing cystic area with hemorrhagic component. Proper target is most proximal portion (red arrow). D. On longitudinal US image, US-CNB was performed at most proximal portion of mass, and this mass was confirmed as undifferentiated pleomorphic sarcoma. PET = positron emission tomography, US = ultrasonography, US-CNB = ultrasound-guided core needle biopsy
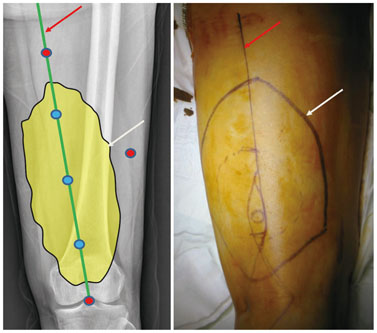
Fig. 3 67-year-old female patient with mass in her right posterior thigh. On radiographic image and actual picture of right upper leg, approximate margin of mass is marked with dark line (white arrows), and there are number of predicted entry points for US-CNB (shown as blue and red dots). Blue dots are located within margins of mass and are included on planned incision line for surgery (red arrows); these are proper needle entry points. In contrast, red dots are located outside of margins of mass, and these are poor needle entry points that could lead to unnecessary resection. US-CNB = ultrasound-guided core needle biopsy
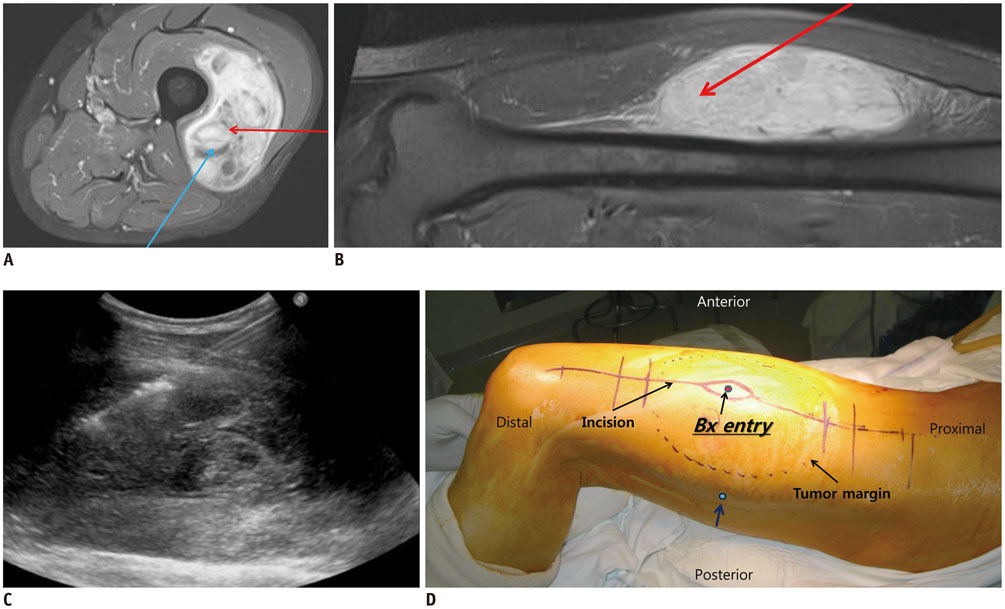
Fig. 4 76-year-old male patient with mass in his left lateral thigh. A, B. On axial (A) and sagittal enhanced T1-weighted images (B), there is heterogeneously enhancing, solid mass that involves vastus intermedius and vastus lateralis muscles. Broadly, two biopsy routes can be considered (as shown by blue and red arrows). Blue route traverses and violates unaffected posterior compartment, but red route crosses only anterior compartment and thus is proper route. C. On longitudinal US image, US-CNB was performed on this mass via red route. D. In actual picture of left upper leg, biopsy entry point was within intended field of surgery and on planned surgery incision line. Imaginary blue biopsy route is marked with blue dots (blue arrow). This mass was confirmed as undifferentiated pleomorphic sarcoma. US = ultrasonography, US-CNB = ultrasound-guided core needle biopsy

Fig. 5 81-year-old female patient with mass in her left upper arm. On axial enhanced T1-weighted image, there is homogeneously enhancing, solid mass that involves biceps brachii muscle. Three biopsy routes can be considered, as shown by blue, green, and red arrows. Blue route crosses uninvolved muscle, and green route could violate median nerve (star) and brachial artery (cross) within mass. Red route does not traverse uninvolved muscular structure and is relatively safe in terms of not violating neurovascular bundle: this is proper route for US-CNB. US-CNB was performed on this mass via red route, and this mass was confirmed as lymphoma. US-CNB = ultrasound-guided core needle biopsy
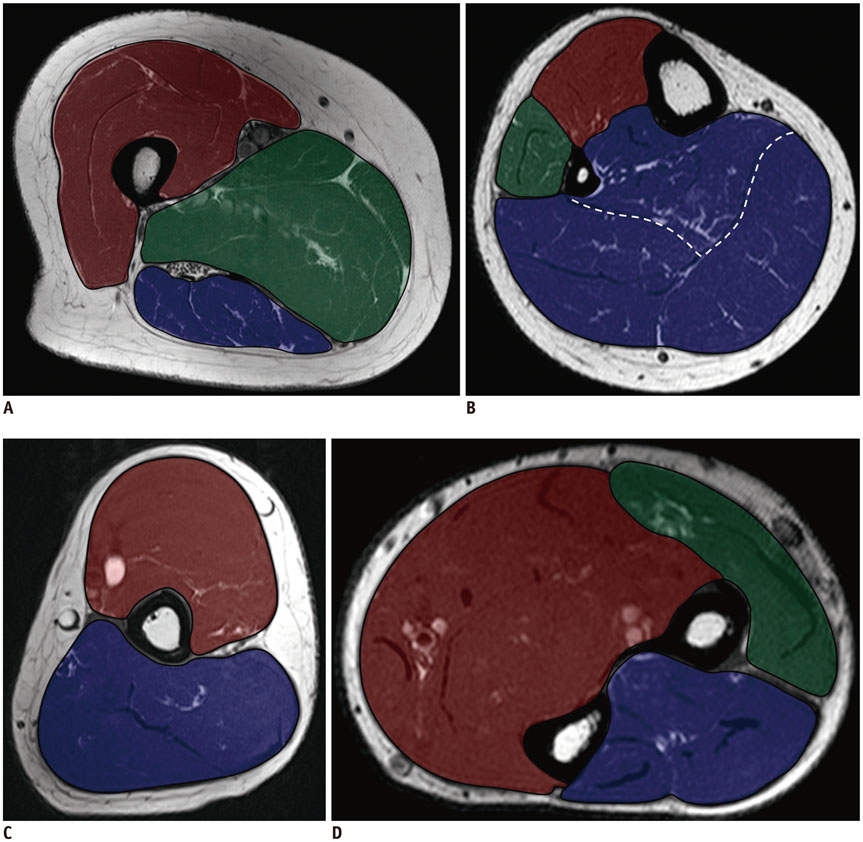
Fig. 6 Compartments of arm and leg. A. Compartments of upper leg. Anterior compartment (red) includes quadriceps muscle group, iliopsoas, sartorius, and tensor fascia lata muscles, and iliotibial band. Medial compartment (green) includes adductor muscle group and gracilis muscle. Posterior compartment (blue) includes hamstring muscle group. B. Compartments of lower leg. Anterior compartment (red) includes tibialis anterior, extensor hallucis longus, and extensor digitorum longus muscles. Lateral compartment (green) includes peroneus longus and brevis muscles. Posterior compartment (blue) includes soleus, gastrocnemius, plantaris, flexor digitorum longus, tibialis posterior, flexor hallucis longus, and popliteus muscles. Posterior compartment can be separated into superficial and deep compartments by transverse intermuscular septum (white dotted line). C. Compartments of upper arm. Anterior compartment (red) includes biceps, brachialis, and coracobrachialis muscles, and posterior compartment (blue) includes triceps muscle. D. Compartments of forearm. In two-compartment description, anterior or flexor compartment (red) is separated from posterior or extensor compartment (blue) by radius, ulna, and intermuscular septum. Using three-compartment classification, three muscles–brachioradialis, extensor carpi radialis longus, and extensor carpi radialis brevis–are considered lateral compartment (green).

Fig. 7 Two types of core biopsy needle. A. Automated core biopsy needle (Acecut; TSK Laboratory, Tochigi, Japan) has both single and two-stage firing options. B. Semiautomated biopsy needle (Stericut; TSK Laboratory). Inner needle of this biopsy system can be introduced by hand for added safety and tactile sensitivity, and needle can be delivered in combination with coaxial introducer needle. C. Manual advancement of inner stylet of semiautomated biopsy needle allows for more delicate control; however, there is higher probability of distally displacing lesion, and thus cannula may partially cut lesion; as result, rest of core tissue would be only adjacent normal tissue.
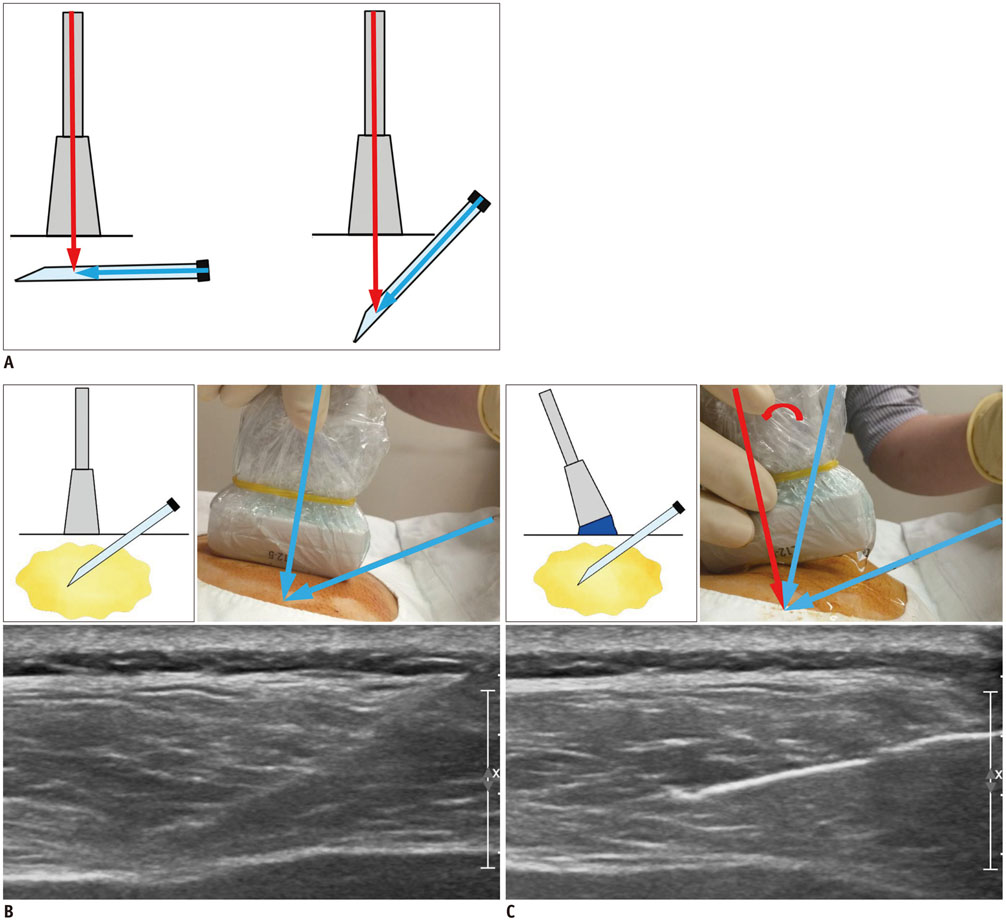
Fig. 8 Conceptual diagram for ultrasonographic visualization of biopsy needle. A. Biopsy needle is better visualized when US beam is steered as close to perpendicular to needle as possible. B. Visualization becomes poor at steep insertion angles because echoes are reflected away from the transducer. C. Heel-and-toe maneuver is performed to bring transducer face into parallel arrangement with needle shaft. US beam will hit perpendicular to needle shaft, thus producing optimal visualization. US = ultrasonography

Fig. 9 Conceptual diagram for US-CNB for small soft tissue lesion. Traversing lesion with core needle may be difficult when lesion is small and mobile. Aiming at center of lesion rather than periphery is helpful for traversing it. US-CNB = ultrasound-guided core needle biopsy
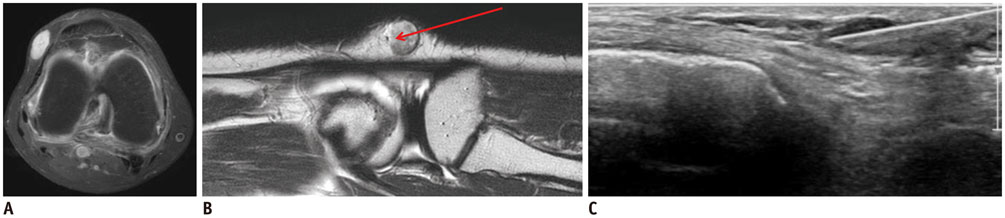
Fig. 10 56-year-old female patient with soft-tissue mass in her left knee. A, B. On axial enhanced T1-weighted (A) and sagittal T2-weighted MR images (B), there is ovoid mass in subcutaneous fat layer of lateral aspect of left knee. This lesion was movable and measured < 0.6 cm in diameter. C. On longitudinal US image, US-CNB was successfully performed via center of lesion, and this lesion was confirmed as myopericytoma. US = ultrasonography, US-CNB = ultrasound-guided core needle biopsy
Cited by 1 articles
-
Core-Needle Biopsy Does Not Show Superior Diagnostic Performance to Fine-Needle Aspiration for Diagnosing Thyroid Nodules
Ilah Shin, Eun-Kyung Kim, Hee Jung Moon, Jung Hyun Yoon, Vivian Youngjean Park, Si Eun Lee, Hye Sun Lee, Jin Young Kwak
Yonsei Med J. 2020;61(2):161-168. doi: 10.3349/ymj.2020.61.2.161.
Reference
-
1. Kim SY, Chung HW. Small musculoskeletal soft-tissue lesions: US-guided core needle biopsy--comparative study of diagnostic yields according to lesion size. Radiology. 2016; 278:156–163.2. Huang AJ, Kattapuram SV. Musculoskeletal neoplasms: biopsy and intervention. Radiol Clin North Am. 2011; 49:1287–1305. vii3. Balach T, Stacy GS, Haydon RC. The clinical evaluation of soft tissue tumors. Radiol Clin North Am. 2011; 49:1185–1196. vi4. Mavrogenis AF, Angelini A, Errani C, Rimondi E. How should musculoskeletal biopsies be performed? Orthopedics. 2014; 37:585–588.5. Toomayan GA, Robertson F, Major NM. Lower extremity compartmental anatomy: clinical relevance to radiologists. Skeletal Radiol. 2005; 34:307–313.6. Toomayan GA, Robertson F, Major NM, Brigman BE. Upper extremity compartmental anatomy: clinical relevance to radiologists. Skeletal Radiol. 2006; 35:195–201.7. Sridharan R, Yunos SM, Aziz S, Hussain RI, Alhabshi SM, Suria Hayati MP, et al. Comparison on the use of semi-automated and automated core biopsy needle in ultrasound guided breast biopsy. Med J Malaysia. 2015; 70:326–333.8. Wu JS, Goldsmith JD, Horwich PJ, Shetty SK, Hochman MG. Bone and soft-tissue lesions: what factors affect diagnostic yield of image-guided core-needle biopsy? Radiology. 2008; 248:962–970.9. Song HS, Kim DY, Yoon KS. Intervention using ultrasonography. J Korean Orthop Assoc. 2013; 48:342–349.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Ultrasound-Fine Needle Aspiration versus Core Biopsy for the Diagnosis of Subepithelial Tumors
- Usefulness of Ultrasound-Guided Automated Core Biopsy of Nonpalpable Breast Lesions
- Fine-Needle Biopsy: Should This Be the First Choice in Endoscopic Ultrasound-Guided Tissue Acquisition?
- Breast Lesions with Discordant Results on Ultrasound-guided Core Needle Biopsy
- Clinical Application of Ultrasound-guided Core Needle Biopsy of the Breast
