Ruptured Corpus Luteal Cyst: Prediction of Clinical Outcomes with CT
- Affiliations
-
- 1Department of Radiology, SMG-SNU Boramae Medical Center, Seoul National University College of Medicine, Seoul 07061, Korea. mmhoan@gmail.com
- 2Department of Obstetrics and Gynecology, SMG-SNU Boramae Medical Center, Seoul National University College of Medicine, Seoul 07061, Korea.
- KMID: 2427229
- DOI: http://doi.org/10.3348/kjr.2017.18.4.607
Abstract
OBJECTIVE
To evaluate the determinant pretreatment CT findings that can predict surgical intervention for patients suffering from corpus luteal cyst rupture with hemoperitoneum.
MATERIALS AND METHODS
From January 2009 to December 2014, a total of 106 female patients (mean age, 26.1 years; range, 17-44 years) who visited the emergency room of our institute for acute abdominal pain and were subsequently diagnosed with ruptured corpus luteal cyst with hemoperitoneum were included in the retrospective study. The analysis of CT findings included cyst size, cyst shape, sentinel clot sign, ring of fire sign, hemoperitoneum depth, active bleeding in portal phase and attenuation of hemoperitoneum. The comparison of CT findings between the surgery and conservative management groups was performed with the Mann-Whitney U test or chi-square test. Logistic regression analysis was used to determine significant CT findings in predicting surgical intervention for a ruptured cyst.
RESULTS
Comparative analysis revealed that the presence of active bleeding and the hemoperitoneum depth were significantly different between the surgery and conservative management groups and were confirmed as significant CT findings for predicting surgery, with adjusted odds ratio (ORs) of 3.773 and 1.318, respectively (p < 0.01). On the receiver-operating characteristic curve analysis for hemoperitoneum depth, the optimal cut-off value was 5.8 cm with 73.7% sensitivity and 58.6% specificity (Az = 0.711, p = 0.004). In cases with a hemoperitoneum depth > 5.8 cm and concurrent active bleeding, the OR for surgery increased to 5.786.
CONCLUSION
The presence of active bleeding and the hemoperitoneum depth on a pretreatment CT scan can be predictive warning signs of surgery for a patient with a ruptured corpus luteal cyst with hemoperitoneum.
MeSH Terms
Figure
-
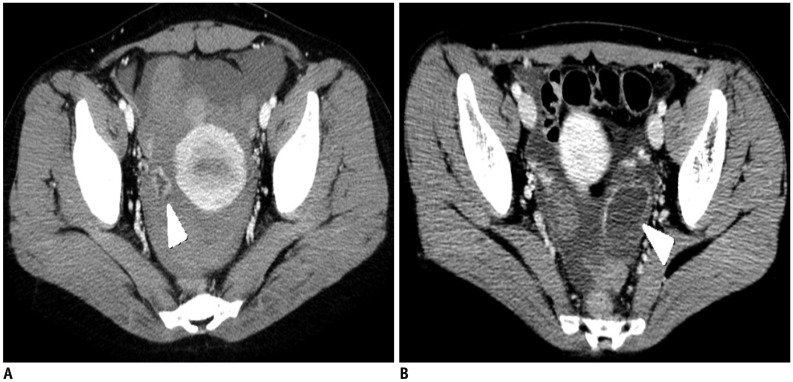
Fig. 1 Sample image of shrunken (A) and tensile (B) shape cysts (arrowheads).
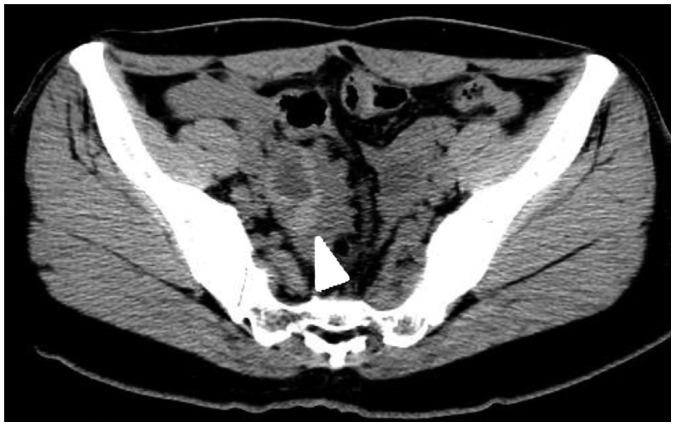
Fig. 2 Sample image of sentinel clot, which was determined as focal high-density clotted blood around ovarian cyst on precontrast CT (arrowhead).

Fig. 3 Sample image of ring of fire sign (arrowhead).Involved cyst also showed tensile contour.
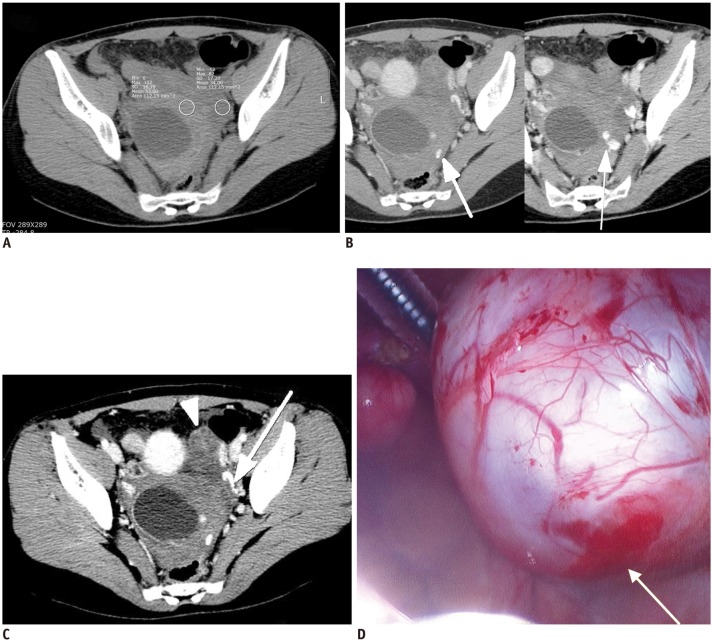
Fig. 4 26-year-old female patient visited emergency room with acute lower abdominal pain.Patient had coitus 3 hours before symptom development.A. Precontrast CT scan showed cystic mass and hemoperitoneum (34–53 HU) in pelvic cavity. B, C. Contrast media extravasation suggestive of active bleeding (arrows) adjacent to cystic mass was detected on portal venous phase axial scans. Two consecutive images confirmed curvilinear lesion as contrast media extravasation, and not dilated paraovarian vein in (B). Left ovary was well-demarcated and intact without active bleeding (arrowhead). D. Patient was surgically treated with right ovarian cystectomy and hematoma evacuation, and active bleeding focus was observed at right ovary (arrow), based on operation record. HU = Hounsfield unit

Fig. 5 ROC analysis for hemoperitoneum depth.Area under curve value was 0.711 (p = 0.004). Optimal cut-off value was 5.8 cm with 75.0% sensitivity and 58.6% specificity. Cut-off value for 95% specificity was 8.75 cm. ROC = receiver-operating characteristic
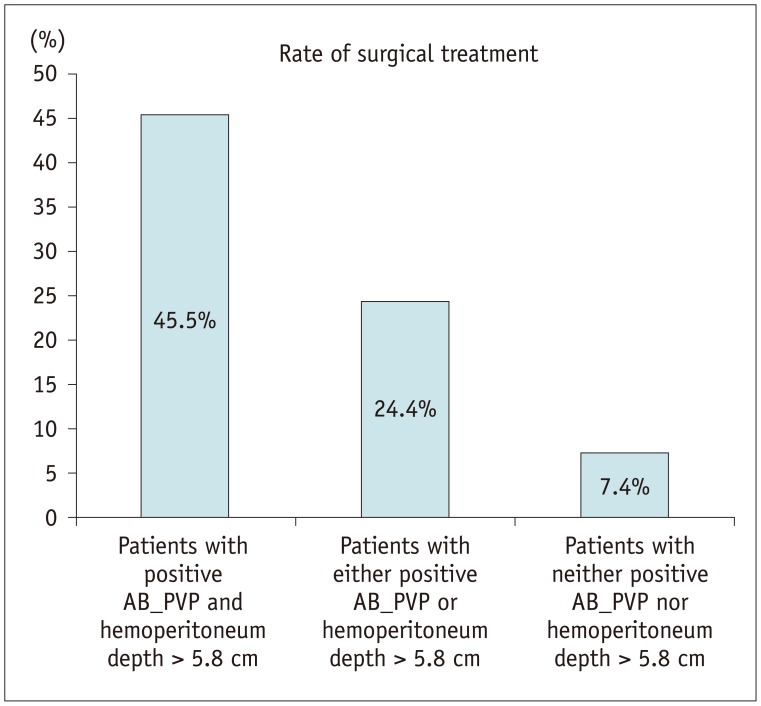
Fig. 6 Rate of surgical treatment based on coexistent CT predictors.AB_PVP = active bleeding in the portal venous phase.
Cited by 1 articles
-
Age of Data in Contemporary Research Articles Published in Representative General Radiology Journals
Ji Hun Kang, Dong Hwan Kim, Seong Ho Park, Jung Hwan Baek
Korean J Radiol. 2018;19(6):1172-1178. doi: 10.3348/kjr.2018.19.6.1172.
Reference
-
1. Teng SW, Tseng JY, Chang CK, Li CT, Chen YJ, Wang PH. Comparison of laparoscopy and laparotomy in managing hemodynamically stable patients with ruptured corpus luteum with hemoperitoneum. J Am Assoc Gynecol Laparosc. 2003; 10:474–477. PMID: 14738631.
Article2. Raziel A, Ron-El R, Pansky M, Arieli S, Bukovsky I, Caspi E. Current management of ruptured corpus luteum. Eur J Obstet Gynecol Reprod Biol. 1993; 50:77–81. PMID: 8365540.
Article3. Bottomley C, Bourne T. Diagnosis and management of ovarian cyst accidents. Best Pract Res Clin Obstet Gynaecol. 2009; 23:711–724. PMID: 19299205.
Article4. Ho WK, Wang YF, Wu HH, Tsai HD, Chen TH, Chen M. Ruptured corpus luteum with hemoperitoneum: case characteristics and demographic changes over time. Taiwan J Obstet Gynecol. 2009; 48:108–112. PMID: 19574168.
Article5. Kim JH, Lee SM, Lee JH, Jo YR, Moon MH, Shin J, et al. Successful conservative management of ruptured ovarian cysts with hemoperitoneum in healthy women. PLoS One. 2014; 9:e91171. PMID: 24608424.
Article6. Choi HJ, Kim SH, Kim SH, Kim HC, Park CM, Lee HJ, et al. Ruptured corpus luteal cyst: CT findings. Korean J Radiol. 2003; 4:42–45. PMID: 12679633.
Article7. Reynolds T, Hill MC, Glassman LM. Sonography of hemorrhagic ovarian cysts. J Clin Ultrasound. 1986; 14:449–453. PMID: 3091645.
Article8. Orwig D, Federle MP. Localized clotted blood as evidence of visceral trauma on CT: the sentinel clot sign. AJR Am J Roentgenol. 1989; 153:747–749. PMID: 2773729.
Article9. Borders RJ, Breiman RS, Yeh BM, Qayyum A, Coakley FV. Computed tomography of corpus luteal cysts. J Comput Assist Tomogr. 2004; 28:340–342. PMID: 15100537.
Article10. Hertzberg BS, Kliewer MA, Paulson EK. Ovarian cyst rupture causing hemoperitoneum: imaging features and the potential for misdiagnosis. Abdom Imaging. 1999; 24:304–308. PMID: 10227900.
Article11. Mohamed M, Al-Ramahi G, McCann M. Postcoital hemoperitoneum caused by ruptured corpus luteal cyst: a hidden etiology. J Surg Case Rep. 2015; 10. 01. DOI: 10.1093/jscr/rjv120. [Epub].
Article12. Wilbur AC, Goldstein LD, Prywitch BA. Hemorrhagic ovarian cysts in patients on anticoagulation therapy: CT findings. J Comput Assist Tomogr. 1993; 17:623–625. PMID: 8331234.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ruptured Corpus Luteal Cyst: CT Findings
- A case of Hyperstimulated Corpus luteal cyst torsion in Pregnancy after In vitro Fertilization
- Corpus Luteum Cyst Rupture - US Findings and Clinical Features
- Agenesis of Corpus Callosum
- Membrane Potential in Luteal Cells from Cyclic Rats: Relationship to Steroidogenic Capacity
