Combined Electrocardiography- and Respiratory-Triggered CT of the Lung to Reduce Respiratory Misregistration Artifacts between Imaging Slabs in Free-Breathing Children: Initial Experience
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea. hwgoo@amc.seoul.kr
- 2Siemens Healthcare, GmbH, Computed Tomography Division, Forchheim 91301, Germany.
- KMID: 2427223
- DOI: http://doi.org/10.3348/kjr.2017.18.5.860
Abstract
OBJECTIVE
Cardiac and respiratory motion artifacts degrade the image quality of lung CT in free-breathing children. The aim of this study was to evaluate the effect of combined electrocardiography (ECG) and respiratory triggering on respiratory misregistration artifacts on lung CT in free-breathing children.
MATERIALS AND METHODS
In total, 15 children (median age 19 months, range 6 months-8 years; 7 boys), who underwent free-breathing ECG-triggered lung CT with and without respiratory-triggering were included. A pressure-sensing belt of a respiratory gating system was used to obtain the respiratory signal. The degree of respiratory misregistration artifacts between imaging slabs was graded on a 4-point scale (1, excellent image quality) on coronal and sagittal images and compared between ECG-triggered lung CT studies with and without respiratory triggering. A p value < 0.05 was considered significant.
RESULTS
Lung CT with combined ECG and respiratory triggering showed significantly less respiratory misregistration artifacts than lung CT with ECG triggering only (1.1 ± 0.4 vs. 2.2 ± 1.0, p = 0.003).
CONCLUSION
Additional respiratory-triggering reduces respiratory misregistration artifacts on ECG-triggered lung CT in free-breathing children.
MeSH Terms
Figure
-
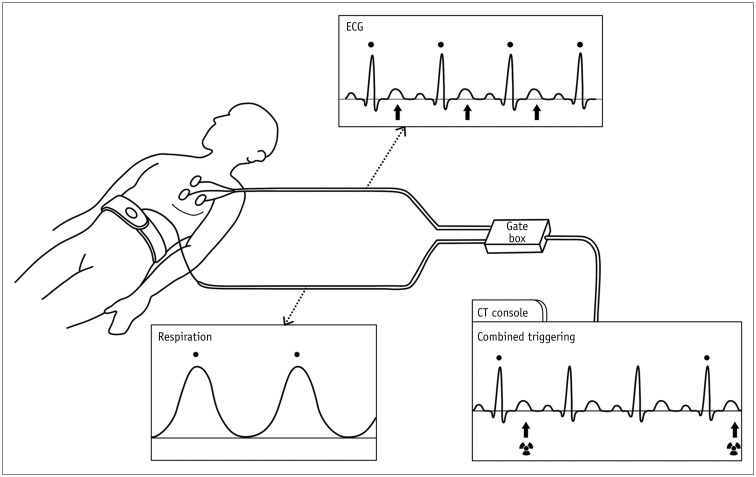
Fig. 1 Schematic drawing of combined ECG and respiratory triggering.From ECG leads, R wave (dot) is detected and end-systolic phase (arrows) is determined by trigger delay. Pressure-sensing belt is placed in upper abdomen to continuously monitor respiratory signal; in this case, respiratory triggering (dot) is produced at inspiration peak. When they occur concurrently, these two triggering signals can be passed through gate box to CT system. Combined ECG and respiratory triggering at R wave on ECG (dot) is displayed on CT console. From combined ECG and respiratory triggering, end-systolic sequential scanning is acquired every three R waves in this case. ECG = electrocardiography
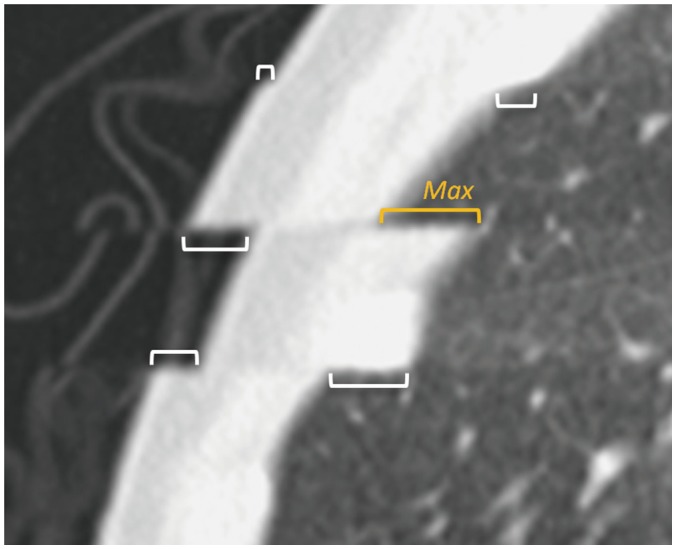
Fig. 2 Measurement of respiratory misregistration artifacts between imaging slabs on sagittal formatted lung CT image.Respiration misregistration occurred at three levels and degree of misregistration was measured in length (brackets) at six locations. Among them, maximal length (Max, orange yellow bracket) was used for semi-quantitative grading (grade 1, < 2 mm; grade 2, 2–5 mm; grade 3, 5–10 mm; and grade 4, > 10 mm).
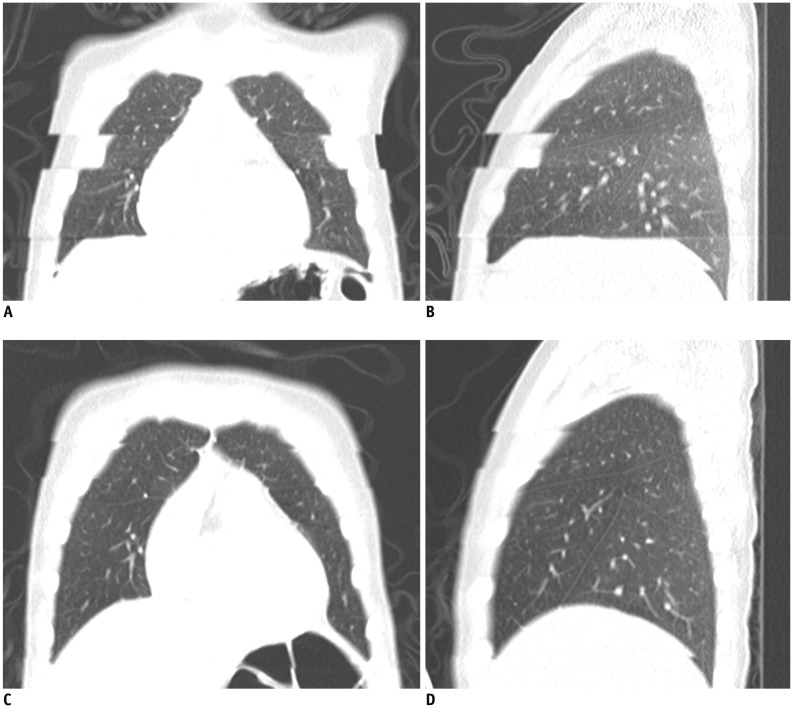
Fig. 3 5-year-old boy with Langerhans cell histiocytosis.A, B. Free-breathing coronal (A) and sagittal (B) ECG-triggered lung CT images acquired at end-systole show grade 4 respiratory misregistration artifacts. C, D. Respiratory misregistration artifacts grade was grade 1 on free-breathing coronal (C) and sagittal (D) lung CT images with combined ECG and respiratory triggering at end-systole and inspiration peak.
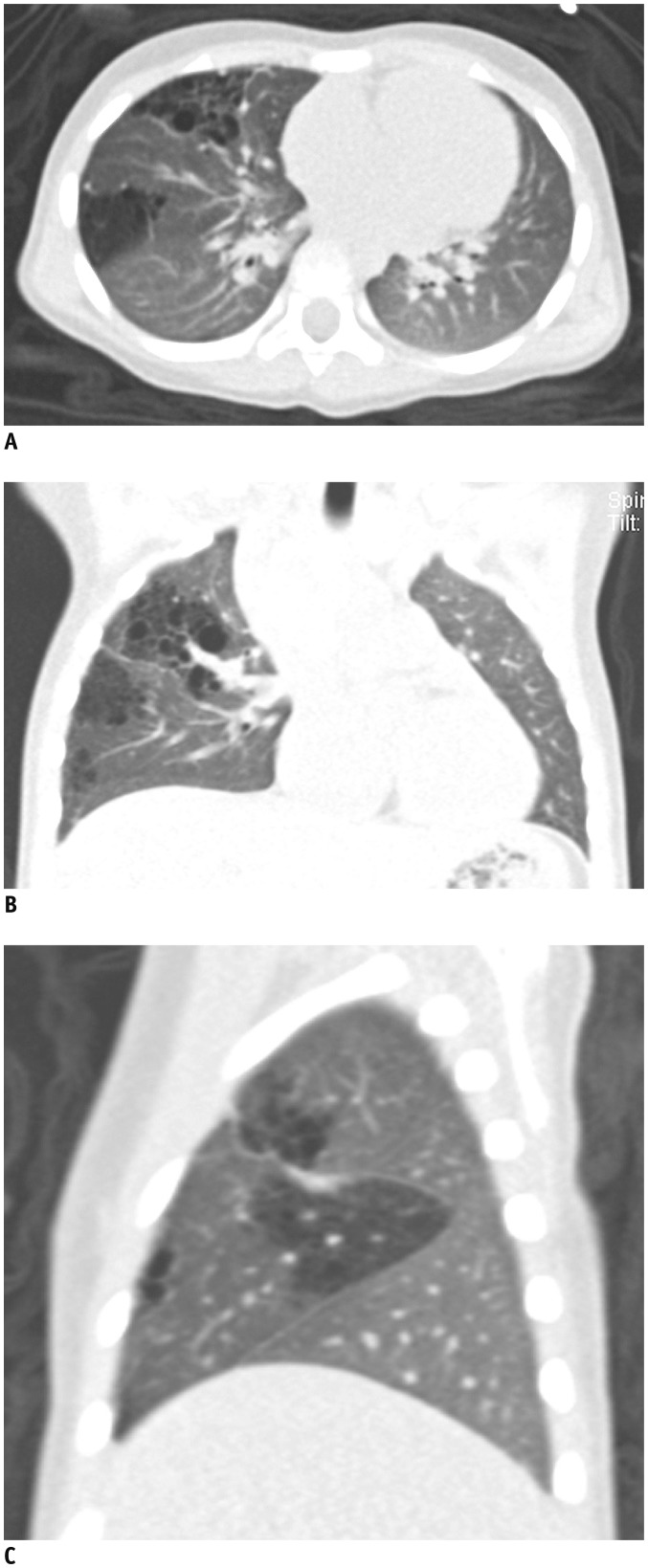
Fig. 4 2-year-old girl with multifocal congenital pulmonary airway malformation.Free-breathing axial (A), coronal (B), and sagittal (C) lung CT images with combined ECG and respiratory triggering at end-systole and expiration peak demonstrate excellent normal anatomic and pathologic details without any motion artifacts.
Cited by 5 articles
-
Four-Dimensional Thoracic CT in Free-Breathing Children
Hyun Woo Goo
Korean J Radiol. 2019;20(1):50-57. doi: 10.3348/kjr.2018.0325.Computed Tomography-Based Ventricular Volumes and Morphometric Parameters for Deciding the Treatment Strategy in Children with a Hypoplastic Left Ventricle: Preliminary Results
Hyun Woo Goo, Sang-Hyub Park
Korean J Radiol. 2018;19(6):1042-1052. doi: 10.3348/kjr.2018.19.6.1042.Age of Data in Contemporary Research Articles Published in Representative General Radiology Journals
Ji Hun Kang, Dong Hwan Kim, Seong Ho Park, Jung Hwan Baek
Korean J Radiol. 2018;19(6):1172-1178. doi: 10.3348/kjr.2018.19.6.1172.Is It Better to Enter a Volume CT Dose Index Value before or after Scan Range Adjustment for Radiation Dose Optimization of Pediatric Cardiothoracic CT with Tube Current Modulation?
Hyun Woo Goo
Korean J Radiol. 2018;19(4):692-703. doi: 10.3348/kjr.2018.19.4.692.Changes in Right Ventricular Volume, Volume Load, and Function Measured with Cardiac Computed Tomography over the Entire Time Course of Tetralogy of Fallot
Hyun Woo Goo
Korean J Radiol. 2019;20(6):956-966. doi: 10.3348/kjr.2018.0891.
Reference
-
1. Montaudon M, Berger P, Blachère H, De Boucaud L, Latrabe V, Laurent F. Thin-section CT of the lung: influence of 0.5-s gantry rotation and ECG triggering on image quality. Eur Radiol. 2001; 11:1681–1687. PMID: 11511889.
Article2. Ha HI, Goo HW, Seo JB, Song JW, Lee JS. Effects of high-resolution CT of the lung using partial versus full reconstruction on motion artifacts and image noise. AJR Am J Roentgenol. 2006; 187:618–622. PMID: 16928921.
Article3. Schoepf UJ, Becker CR, Bruening RD, Helmberger T, Staebler A, Leimeister P, et al. Electrocardiographically gated thin-section CT of the lung. Radiology. 1999; 212:649–654. PMID: 10478227.
Article4. Nishiura M, Johkoh T, Yamamoto S, Honda O, Kozuka T, Koyama M, et al. Electrocardiography-triggered high-resolution CT for reducing cardiac motion artifact: evaluation of the extent of ground-glass attenuation in patients with idiopathic pulmonary fibrosis. Radiat Med. 2007; 25:523–528. PMID: 18085403.
Article5. Kalender WA, Rienmüller R, Seissler W, Behr J, Welke M, Fichte H. Measurement of pulmonary parenchymal attenuation: use of spirometric gating with quantitative CT. Radiology. 1990; 175:265–268. PMID: 2315492.
Article6. Mori M, Murata K, Takahashi M, Shimoyama K, Ota T, Morita R, et al. Accurate contiguous sections without breath-holding on chest CT: value of respiratory gating and ultrafast CT. AJR Am J Roentgenol. 1994; 162:1057–1062. PMID: 8165981.
Article7. Robinson TE, Leung AN, Moss RB, Blankenberg FG, al-Dabbagh H, Northway WH. Standardized high-resolution CT of the lung using a spirometer-triggered electron beam CT scanner. AJR Am J Roentgenol. 1999; 172:1636–1638. PMID: 10350305.
Article8. Zaporozhan J, Ley S, Unterhinninghofen R, Saito Y, Fabel-Schulte M, Keller S, et al. Free-breathing three-dimensional computed tomography of the lung using prospective respiratory gating: charge-coupled device camera and laser sensor device in an animal experiment. Invest Radiol. 2006; 41:468–475. PMID: 16625110.9. Long FR, Castile RG, Brody AS, Hogan MJ, Flucke RL, Filbrun DA, et al. Lungs in infants and young children: improved thin-section CT with a noninvasive controlled-ventilation technique--initial experience. Radiology. 1999; 212:588–593. PMID: 10429722.
Article10. Long FR, Castile RG. Technique and clinical applications of full-inflation and end-exhalation controlled-ventilation chest CT in infants and young children. Pediatr Radiol. 2001; 31:413–422. PMID: 11436888.
Article11. Mueller KS, Long FR, Flucke RL, Castile RG. Volume-monitored chest CT: a simplified method for obtaining motion-free images near full inspiratory and end expiratory lung volumes. Pediatr Radiol. 2010; 40:1663–1669. PMID: 20508926.
Article12. Lee EY, Mason KP, Zurakowski D, Waltz DA, Ralph A, Riaz F, et al. MDCT assessment of tracheomalacia in symptomatic infants with mediastinal aortic vascular anomalies: preliminary technical experience. Pediatr Radiol. 2008; 38:82–88. PMID: 18038169.
Article13. Ritchie CJ, Godwin JD, Crawford CR, Stanford W, Anno H, Kim Y. Minimum scan speeds for suppression of motion artifacts in CT. Radiology. 1992; 185:37–42. PMID: 1523332.
Article14. Thiyagarajan R, Sinha SN, Ravichandran R, Samuvel K, Yadav G, Sigamani AK, et al. Respiratory gated radiotherapy-pretreatment patient specific quality assurance. J Med Phys. 2016; 41:65–70. PMID: 27051173.
Article15. Werner MK, Parker JA, Kolodny GM, English JR, Palmer MR. Respiratory gating enhances imaging of pulmonary nodules and measurement of tracer uptake in FDG PET/CT. AJR Am J Roentgenol. 2009; 193:1640–1645. PMID: 19933659.
Article16. Ley S, Ley-Zaporozhan J, Unterhinninghofen R, Saito Y, Fabel-Schulte M, Weinheimer O, et al. Investigation of retrospective respiratory gating techniques for acquisition of thin-slice 4D-multidetector-computed tomorgraphy (MDCT) of the lung: feasibility study in a large animal model. Exp Lung Res. 2006; 32:395–412. PMID: 17162648.
Article17. Behzadi C, Groth M, Henes FO, Schwarz D, Deibele A, Begemann PG, et al. Intraindividual comparison of image quality using retrospective and prospective respiratory gating for the acquisition of thin sliced four dimensional multidetector CT of the thorax in a porcine model. Exp Lung Res. 2015; 41:489–498. PMID: 26495957.
Article18. Oechsner M, Pracht ED, Staeb D, Arnold JF, Köstler H, Hahn D, et al. Lung imaging under free-breathing conditions. Magn Reson Med. 2009; 61:723–727. PMID: 19097250.
Article19. Teräs M, Kokki T, Durand-Schaefer N, Noponen T, Pietilä M, Kiss J, et al. Dual-gated cardiac PET-clinical feasibility study. Eur J Nucl Med Mol Imaging. 2010; 37:505–516. PMID: 19789872.
Article20. Goo HW, Yang DH. Coronary artery visibility in free-breathing young children with congenital heart disease on cardiac 64-slice CT: dual-source ECG-triggered sequential scan vs. single-source non-ECG-synchronized spiral scan. Pediatr Radiol. 2010; 40:1670–1680. PMID: 20464385.
Article21. Goo HW. Current trends in cardiac CT in children. Acta Radiol. 2013; 54:1055–1062. PMID: 23104372.
Article22. Goo HW. Individualized volume CT dose index determined by cross-sectional area and mean density of the body to achieve uniform image noise of contrast-enhanced pediatric chest CT obtained at variable kV levels and with combined tube current modulation. Pediatr Radiol. 2011; 41:839–847. PMID: 21656275.
Article23. Goo HW. CT radiation dose optimization and estimation: an update for radiologists. Korean J Radiol. 2012; 13:1–11. PMID: 22247630.
Article24. Lell MM, Scharf M, Eller A, Wuest W, Allmendinger T, Fuchs F, et al. Feasibility of respiratory-gated high-pitch spiral CT: free-breathing inspiratory image quality. Acad Radiol. 2016; 23:406–412. PMID: 26853970.25. Bae KT. Peak contrast enhancement in CT and MR angiography: when does it occur and why? Pharmacokinetic study in a porcine model. Radiology. 2003; 227:809–816. PMID: 12702823.
Article26. Goo HW. State-of-the-art CT imaging techniques for congenital heart disease. Korean J Radiol. 2010; 11:4–18. PMID: 20046490.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Misregistration Artifact due to Respiratory Motion on Spiral CT of the Liver
- Development of Respiratory Training System Using Individual Characteristic Guiding Waveform
- Four-Dimensional Thoracic CT in Free-Breathing Children
- Detection of Hepatic Lesion: Comparison of Free-Breathing and Respiratory-Triggered Diffusion-Weighted MR imaging on 1.5-T MR system
- Recurrent Paroxysmal Atrial Tachycardia Triggered by Deep Inspiration During Contrast Enhanced Computed Tomography Coronary Angiography
