Coronary Stent Infection Presented as Recurrent Stent Thrombosis
- Affiliations
-
- 1Division of Interventional Cardiology, Cardiovascular Center, Taichung Veterans General Hospital, Taichung, Taiwan, R.O.C. wcchangvghtc@gmail.com
- 2School of Medicine, National Yang-Ming University, Taipei, Taiwan, R.O.C.
- 3Division of Cardiovascular Surgery, Department of Surgery, Feng Yuan Hospital, Taichung, Taiwan, R.O.C.
- KMID: 2427138
- DOI: http://doi.org/10.3349/ymj.2017.58.2.458
Abstract
- Percutaneous transluminal coronary angioplasty with metal stent placement has become a well-developed treatment modality for coronary stenotic lesions. Although infection involving implanted stents is rare, it can, however, occur with high morbidity and mortality. We describe herein a case of an inserted coronary stent that was infected and complicated with recurrent stent thrombosis, pseudoaneurysm formation and severe sepsis. Despite repeated intervention and bypass surgery, the patient died from severe sepsis.
MeSH Terms
Figure
-

Fig. 1 Serial angiography of first time intervention. (A) Right oblique caudal view of left coronary artery shows severe stenosis of distal left main (LM, arrow) and proximal left circumflex artery. (B) Diffuse stenosis and distal total occlusion of right coronary artery (RCA). (C) Angiography of RCA after stenting. (D) Stent deployed from LM to proximal left anterior descending artery (arrow). (E) Right oblique caudal view of left coronary artery after stenting (arrow: LM stenting). (F) Spider view of left coronary artery after stenting.
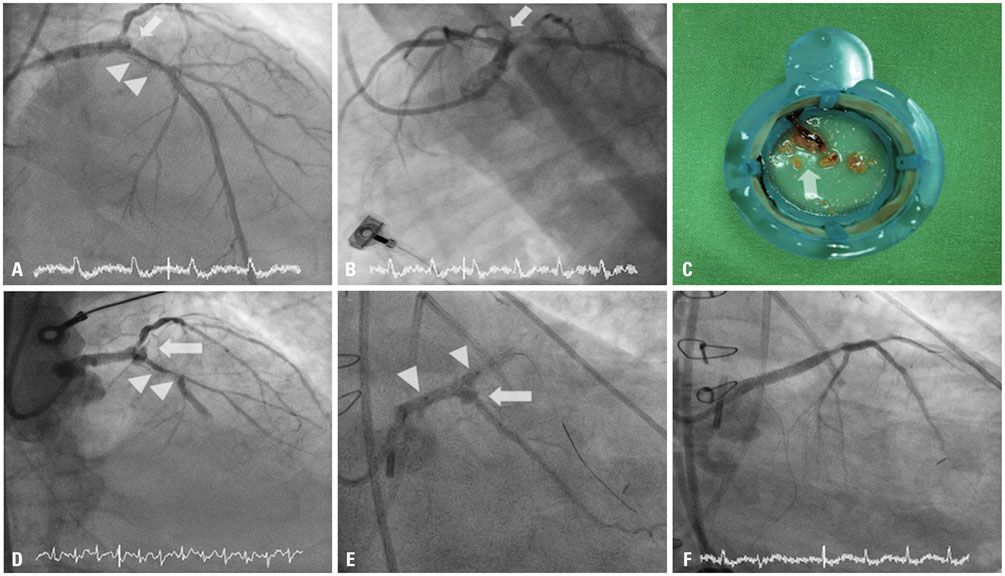
Fig. 2 (A, B, and C) Emergent angioplasty for first time stent thrombosis. (D) Emergent angioplasty for second time stent thrombosis. (E and F) Putting a graft stent. (A) Right oblique cranial view of left coronary artery shows stent thrombosis in proximal LAD (arrowheads) and pseudoaneurysm in distal LM (arrow). (B) Spider view of left coronary artery shows coronary pseudoaneurysm in distal LM (arrow). (C) Material from manual thrombus aspirator reveals thrombi with pus like material (arrow). (D) One day later, emergent angiography shows recurrent in stent thrombosis (arrowheads) and progression of coronary pseudoaneurysm in distal LM (arrow). (E) Graft stent being inserted from LM to proximal LAD (stent margin marked as arrowheads) to cover coronary pseudoaneurysm (arrow). (F) After inserting graft stent, angiography of left coronary artery reveals complete jailing of LCX. LAD, left anterior descending artery; LM, left main; LCX, left circumflex artery.
Reference
-
1. Bosman WM, Borger van der Burg BL, Schuttevaer HM, Thoma S, Hedeman Joosten PP. Infections of intravascular bare metal stents: a case report and review of literature. Eur J Vasc Endovasc Surg. 2014; 47:87–99.
Article2. Roubelakis A, Rawlins J, Baliulis G, Olsen S, Corbett S, Kaarne M, et al. Coronary artery rupture caused by stent infection: a rare complication. Circulation. 2015; 131:1302–1303.3. Wu EB, Chan WW, Yu CM. Left main stem rupture caused by methicillin resistant Staphylococcus aureus infection of left main stent treated by covered stenting. Int J Cardiol. 2010; 144:e39–e41.
Article4. Garg RK, Sear JE, Hockstad ES. Spontaneous coronary artery perforation secondary to a sirolimus-eluting stent infection. J Invasive Cardiol. 2007; 19:E303–E306.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrent Stent Thrombosis in Different Coronary Arteries
- Coincidental Occurrence of Acute In-stent Thrombosis and Iatrogenic Vessel Perforation During a Wingspan Stent Placement: Management with a Stent In-stent Technique
- Recurrent Very Late Stent Thrombosis in a Systemic Lupus Erythematous Patient
- Risk of Stent Stenosis after Implanting a First-Generation Drug-Eluting Stent and Drug Balloon Angioplasty
- Drug-Eluting Stent Used to Treat a Case of Recurrent Right Coronary Artery In-Stent Restenoses often Accompanied by Acute Inferior Wall Myocardial Infarction
