Clin Endosc.
2013 Jul;46(4):384-389.
Angular Positioning of Stent Increases Bowel Perforation after Self-Expandable Metal Stent Placement for Malignant Colorectal Obstruction
- Affiliations
-
- 1Digestive Disease Center, CHA Bundang Medical Center, CHA University, Seongnam, Korea. sphong@cha.ac.kr
Abstract
- BACKGROUND/AIMS
Some factors like stent wires, balloon dilatation and use of guide wires seems to increase perforation after self-expandable metal stent (SEMS) placement, but few studies mentioned about the relationship between angulation of malignant stricture and perforation. The present study aimed to confirm that more angular positioning of stents increases perforation.
METHODS
This study was conducted with retrospectively evaluation at Digestive Disease Center, CHA Bundang Medical Center, CHA University. Between January 2002 and August 2011, SEMS was inserted in 130 patients with malignant colorectal obstruction. We studied the difference in the angle of stenosis between perforation and non-perforation groups using fluorography images.
RESULTS
SEMS insertion was performed in 130 cases of obstruction due to colon cancer. Perforation occurred in eight patients (6.2%) of them. Thirteen cases were excluded from the analysis due to poor fluoroscopic images. Among the eight patients with perforation, the mean stenosis angle was 109.9degrees compared to 153.1degrees in the nonperforation group, indicating that the angle was more acute in the perforation group (p=0.016).
CONCLUSIONS
This study shows that more angular positioning of stent increases bowel perforation after SEMS placement for malignant colorectal obstruction.
MeSH Terms
Figure
-
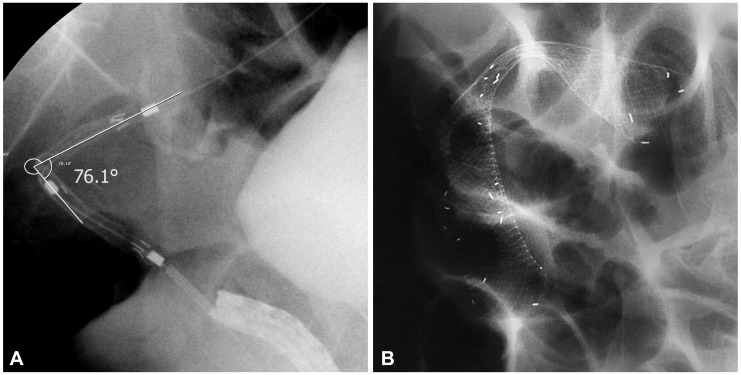
Fig. 1 Fluoroscopic images of the stenotic lesion during stent insertion. (A) The angle of malignant stenosis was 76°. (B) A full-covered metallic stent was inserted, and perforation occurred in 1 day.
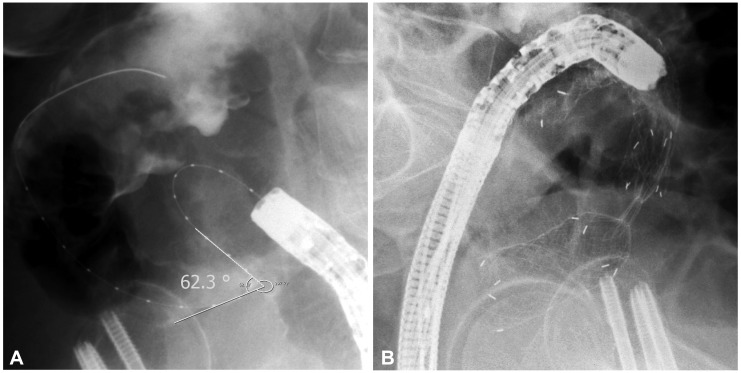
Fig. 2 Fluoroscopic images of the stenotic lesion during stent insertion. (A) The angle of malignant stenosis was 62°. (B) Two uncovered metallic stents were placed to each proximal and distal portion of the stenosis and overlapped at the bent. Perforation was developed in 3 days.
Reference
-
1. Dohmoto M, Hünerbein M, Schlag PM. Application of rectal stents for palliation of obstructing rectosigmoid cancer. Surg Endosc. 1997; 11:758–761. PMID: 9214327.
Article2. Deans GT, Krukowski ZH, Irwin ST. Malignant obstruction of the left colon. Br J Surg. 1994; 81:1270–1276. PMID: 7953385.
Article3. Wang HS, Lin JK, Mou CY, et al. Long-term prognosis of patients with obstructing carcinoma of the right colon. Am J Surg. 2004; 187:497–500. PMID: 15041498.
Article4. Barillari P, Aurello P, De Angelis R, et al. Management and survival of patients affected with obstructive colorectal cancer. Int Surg. 1992; 77:251–255. PMID: 1335999.5. Karadağ A, Menteş BB, Uner A, Irkörücü O, Ayaz S, Ozkan S. Impact of stomatherapy on quality of life in patients with permanent colostomies or ileostomies. Int J Colorectal Dis. 2003; 18:234–238. PMID: 12673489.
Article6. Khot UP, Lang AW, Murali K, Parker MC. Systematic review of the efficacy and safety of colorectal stents. Br J Surg. 2002; 89:1096–1102. PMID: 12190673.
Article8. Baron TH. Expandable metal stents for the treatment of cancerous obstruction of the gastrointestinal tract. N Engl J Med. 2001; 344:1681–1687. PMID: 11386268.
Article9. Sebastian S, Johnston S, Geoghegan T, Torreggiani W, Buckley M. Pooled analysis of the efficacy and safety of self-expanding metal stenting in malignant colorectal obstruction. Am J Gastroenterol. 2004; 99:2051–2057. PMID: 15447772.
Article10. Song HY, Kim JH, Shin JH, et al. A dual-design expandable colorectal stent for malignant colorectal obstruction: results of a multicenter study. Endoscopy. 2007; 39:448–454. PMID: 17516352.
Article11. Song HY, Kim JH, Kim KR, et al. Malignant rectal obstruction within 5 cm of the anal verge: is there a role for expandable metallic stent placement. Gastrointest Endosc. 2008; 68:713–720. PMID: 18561924.
Article12. Binkert CA, Ledermann H, Jost R, Saurenmann P, Decurtins M, Zollikofer CL. Acute colonic obstruction: clinical aspects and cost-effectiveness of preoperative and palliative treatment with self-expanding metallic stents: a preliminary report. Radiology. 1998; 206:199–204. PMID: 9423673.13. Saida Y, Sumiyama Y, Nagao J, Takase M. Stent endoprosthesis for obstructing colorectal cancers. Dis Colon Rectum. 1996; 39:552–555. PMID: 8620807.
Article14. Lopera JE, De Gregorio MA. Fluoroscopic management of complications after colorectal stent placement. Gut Liver. 2010; 4(Suppl 1):S9–S18. PMID: 21103302.
Article15. Camúñez F, Echenagusia A, Simó G, Turégano F, Vázquez J, Barreiro-Meiro I. Malignant colorectal obstruction treated by means of self-expanding metallic stents: effectiveness before surgery and in palliation. Radiology. 2000; 216:492–497. PMID: 10924576.
Article16. Cho YK, Kim SW, Lee BI, et al. Clinical outcome of self-expandable metal stent placement in the management of malignant proximal colon obstruction. Gut Liver. 2011; 5:165–170. PMID: 21814596.
Article17. Small AJ, Baron TH. Comparison of Wallstent and Ultraflex stents for palliation of malignant left-sided colon obstruction: a retrospective, case-matched analysis. Gastrointest Endosc. 2008; 67:478–488. PMID: 18294511.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fluoroscopic Stent Placement as a Bridge to Surgery for Malignant Colorectal Obstruction: Short- and Long-Term Outcomes
- Percutaneous Enteral Stent Placement Using a Transhepatic Access for Palliation of Malignant Bowel Obstruction after Surgery
- Endoscopic Management of Malignant Colonic Obstruction
- A Dual Expandable Stent for Treatment of Malignant Colorectal Obstruction: Long-Term Follow-Up Results
- Colonic Stent-Related Complications and Their Management
