Investigation of Symptomatic Unstable Changes of Non-Fused Component in the Mixed-Type Cervical Ossification of Posterior Longitudinal Ligament Using Dynamic Magnetic Resonance Imaging: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Yeungnam University Medical Center, Yeungnam University College of Medicine, Daegu, Korea. jicns@ynu.ac.kr
- KMID: 2424333
- DOI: http://doi.org/10.13004/kjnt.2018.14.2.164
Abstract
- A 43-year-old man was transferred to our hospital with recurring myelopathic symptoms after previous anterior and posterior surgical decompressions for mixed-type cervical ossification of the posterior longitudinal ligament (OPLL). Conventional magnetic resonance imaging (MRI) showed a preserved cervical curve and the achievement of successful decompression after the previous surgeries. The patient's symptoms were aggravated when he was in the extended neck posture. Dynamic MRI performed with the patient in an extended neck position revealed cord compression by OPLL from C3 to C4 with newly developed retrolisthesis of the C4-5 segment. We recommend the use of dynamic MRI to investigate motion-dependent cord compression caused by instability of the non-fused OPLL component.
MeSH Terms
Figure
-
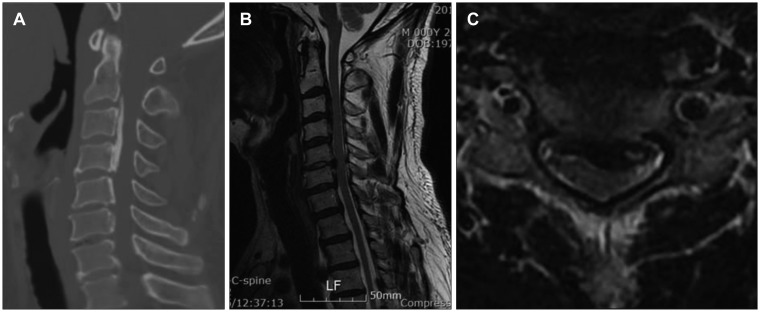
FIGURE 1 (A) Computed tomography scan and (B, C) magnetic resonance imaging reveal cord compression by ossification of the posterior longitudinal ligament (OPLL) from C2 to C6 with a mixed type (non-fused segment on C4–5). The cord is most severely compressed by OPLL and the protruded disc on C5–6 segment.
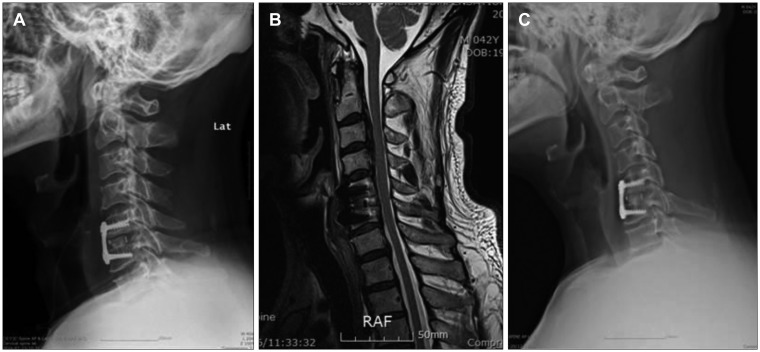
FIGURE 2 (A) There was a temporary neurological improvement following the first surgery. (B) However, the patient complained of newly developed urinary incontinence and upper motor weakness with progressing gait disturbance 1 month postoperatively. On follow-up magnetic resonance imaging, (C) there was sustained cord compression on C3 to C5. Decompressive laminectomy was performed to decompress the cervical cord on C3 to C5.
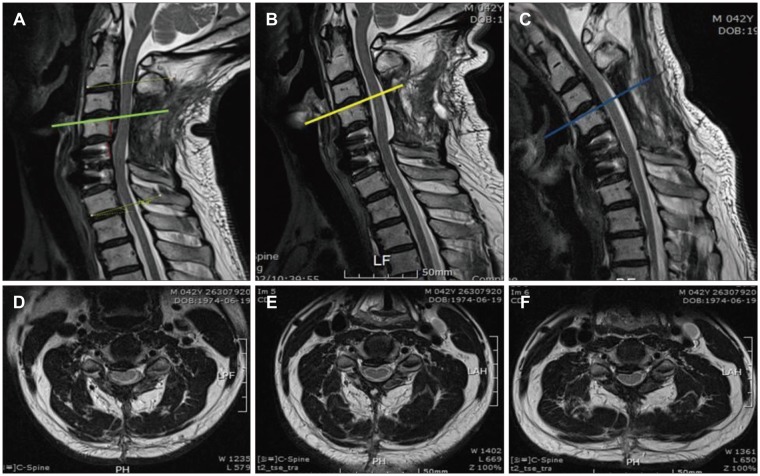
FIGURE 3 (A, D) Dynamic magnetic resonance imaging (MRI) on the extended neck posture revealed cord compression with obliteration of ventral cerebrospinal fluid (CSF) space from the C3 to C4 levels by ossification of the posterior longitudinal ligament (OPLL) with newly developed retrolisthesis of the C4–5 segment. There was no definite compressive effect of the posterior paraspinal muscles. (B, E) MRI of neutral neck posture shows no cord compression by OPLL and the posterior paraspinal muscles. (C, F) On the flexed neutral neck postures, cord compression is partially suspected on the axial view. There is slight amount of pressure on the cord without obliteration of ventral CSF space compared to extended neck posture.
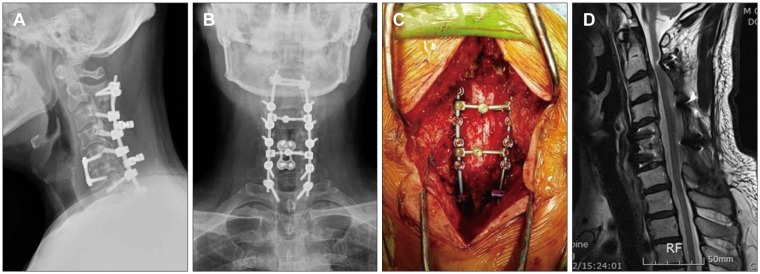
FIGURE 4 (A–C) Additional decompressive laminectomy was performed on the C6 and C7 levels with excoriation of adherent tissue around the previous laminectomy site, and then posterior screw fixation was done from C2 to T1 by placing a dome-shaped crosslink to prevent cord compression by the posterior stuructures. (D) After 18 months of follow-up, there was no cord compression either anteriorly and posteriorly on magnetic resonance imaging.
Reference
-
1. An HS, Al-Shihabi L, Kurd M. Surgical treatment for ossification of the posterior longitudinal ligament in the cervical spine. J Am Acad Orthop Surg. 2014; 22:420–429. PMID: 24966248.
Article2. Chiba K, Yamamoto I, Hirabayashi H, Iwasaki M, Goto H, Yonenobu K, et al. Multicenter study investigating the postoperative progression of ossification of the posterior longitudinal ligament in the cervical spine: a new computer-assisted measurement. J Neurosurg Spine. 2005; 3:17–23. PMID: 16122017.
Article3. Dalbayrak S, Yaman O, Firidin MN, Yilmaz T, Yilmaz M. The contribution of cervical dynamic magnetic resonance imaging to the surgical treatment of cervical spondylotic myelopathy. Turk Neurosurg. 2015; 25:36–42. PMID: 25640543.4. Evans LT, Lollis SS. Dynamic compression of the spinal cord by paraspinal muscles following cervical laminectomy: Diagnosis using flexion-extension MRI. Case Rep Radiol. 2015; 2015:275623. PMID: 25984378.
Article5. Jeon I, Cho YE. Analysis of factors contributing to repeat surgery in multi-segments cervical ossification of posterior longitudinal ligament. J Korean Neurosurg Soc. 2018; 61:224–232. PMID: 29526066.
Article6. Kawaguchi Y, Kanamori M, Ishihara H, Nakamura H, Sugimori K, Tsuji H, et al. Progression of ossification of the posterior longitudinal ligament following en bloc cervical laminoplasty. J Bone Joint Surg Am. 2001; 83-A:1798–1802. PMID: 11741057.
Article7. Lee DH, Cho JH, Kim NH, Kim S, Choi J, Hwang CJ, et al. Radiological risk factors for progression of ossification of posterior longitudinal ligament following laminoplasty. Spine J. 2018; 18:1116–1121. PMID: 29126953.
Article8. Sheen JJ, Jeon SR. Midline splitting cervical laminoplasty using allogeneic bone spacers: Comparison of fusion rates between cervical spondylotic myelopathy and ossification of posterior longitudinal ligament. Korean J Neurotrauma. 2014; 10:60–65. PMID: 27169035.
Article9. Smith ZA, Buchanan CC, Raphael D, Khoo LT. Ossification of the posterior longitudinal ligament: pathogenesis, management, and current surgical approaches. A review. Neurosurg Focus. 2011; 30:E10.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cervical Ossification of Posterior Longitudinal Ligament in X-Linked Hypophosphatemic Rickets Revealing Homogeneously Increased Vertebral Bone Density
- Ossification of the Posterior Longitudinal Ligament: 2 cases report
- Dysphagia Caused by Ossification of the Cervical Anterior Longitudinal Ligament
- Ossification of Posterior Longitudinal Ligament(OPLL) of Cervical Spine
- Cervical Spine CT and MRI Findings in a Patient with Ossification of the Posterior Longitudinal Ligament
