Advanced Pediatric Kienbock's Disease
- Affiliations
-
- 1Department of Orthopedic Surgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea. dhkim1149@gmail.com
- KMID: 2424106
- DOI: http://doi.org/10.4055/jkoa.2018.53.5.453
Abstract
- Kienbock's disease is very rare in pediatrics. The treatment of Kienbock's disease is controversial and depends on an understanding of the natural history of the disease. The methods proposed vary from conservative treatment to surgical treatment such as radial shortening or scaphotrapezoidal joint fixation, but there are few therapeutic guidelines for paediatric Kienbock's disease. We encountered a 14-year-old male with Lichtman stage IIIB disease and treated him with conservative management. We report this rare case of advanced paediatric Kienbock's disease with good clinical results at the 2-year follow-up along with a review of the relevant literature.
Keyword
Figure
-

Figure 1 A 14-year-old male with wrist pain due to stage IIIA Kienbock's disease. Standard anteroposterior and lateral radiographs at presentation show that the lunate has sclerotic changes with a collapse of height. A neutral ulnar variance can be seen.

Figure 2 (A) Sagittal computed tomography image shows bony fragmentation of the lunate bone. (B) Coronal T1-weighted magnetic resonance imaging (MRI) shows diffuse hypointensity of the lunate bone. Coronal T2-weighted fat-suppressed MRI shows diffuse hyperintensity and collapse of the lunate bone.

Figure 3 Anteroposterior and lateral radiographs at 12 weeks after casting. The carpal height ratio did not change, and the collapse of the lunate did not progress.

Figure 4 Twenty-four months after the cast was removed, the patient reported a resolution of their wrist pain and showed a preservation of some wrist motions.
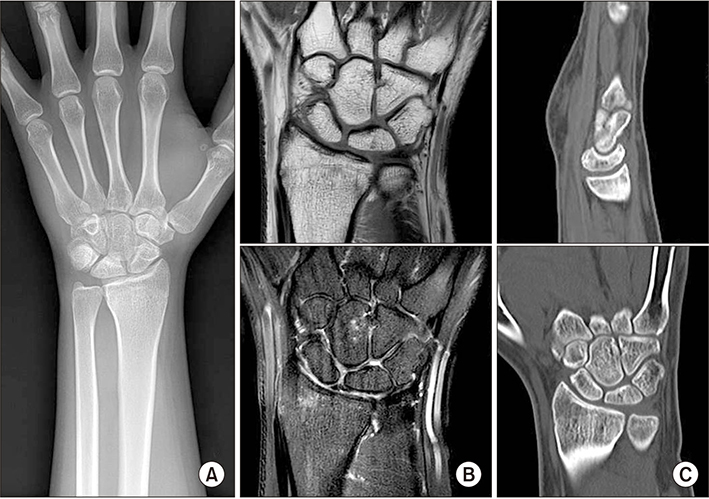
Figure 5 Radiograph (A), magnetic resonance imaging (B) and computed tomography (C) at the last follow-up evaluation showed no recurrence of Kienbock's disease.
Reference
-
1. Ferlic RJ, Lee DH, Lopez-Ben RR. Pediatric Kienböck's disease: case report and review of the literature. Clin Orthop Relat Res. 2003; (408):237–244.
Article2. Cvitanich M, Solomons M. Juvenile lunatomalacia is this Kienböck's disease? J Hand Surg Br. 2004; 29:288–292.3. Kazuki K, Uemura T, Okada M, Egi T. Time course of magnetic resonance images in an adolescent patient with Kienböck's disease treated by temporary scaphotrapezoidal joint fixation: a case report. J Hand Surg Am. 2006; 31:63–67.
Article4. Kim TY, Culp RW, Osterman AL, Bednar JM. Kienbock's disease in children. Jefferson Orthopedic J. 1997; 25:53–57.5. Irisarri C, Kalb K, Ribak S. Infantile and juvenile lunatomalacia. J Hand Surg Eur Vol. 2010; 35:544–548.
Article6. Greene WB. Kienböck disease in a child who has cerebral palsy. A case report. J Bone Joint Surg Am. 1996; 78:1568–1573.
Article7. Herzberg G, Mercier S, Charbonnier JP, Got P. Kienböck's disease in a 14-year-old gymnast: a case report. J Hand Surg Am. 2006; 31:264–268.
Article8. Iwasaki N, Minami A, Ishikawa J, Kato H, Minami M. Radial osteotomies for teenage patients with Kienböck disease. Clin Orthop Relat Res. 2005; 439:116–122.
Article9. Yajima H, Ono H, Tamai S. Temporary internal fixation of the scaphotrapezio-trapezoidal joint for the treatment of Kienböck's disease: a preliminary study. J Hand Surg Am. 1998; 23:402–410.
Article10. Herdem M, Ozkan C, Bayram H. Overgrowth after radial shortening for Kienböck's disease in a teenager: case report. J Hand Surg Am. 2006; 31:1322–1325.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rupture of the Extensor Tendon Secondary to Advanced Kienbock's Disease
- Treatment of Kienbock's Disease Using Fascia Latae: Two Cases Report
- Ulnar Lengthening in the Treatment of Kienbock's Disease
- A comparative study of the surgical procedures to treat advanced Kienbock's disease
- Roles and Limitations of Arthroscopy in the Treatment of Kienböck’s Disease
