Neurointervention.
2018 Mar;13(1):48-53. 10.5469/neuroint.2018.13.1.48.
Diagnosis of Cerebral Aneurysm Via Magnetic Resonance Angiography Screening: Emphasis on Legal Responsibility Increases False Positive Rate
- Affiliations
-
- 1Department of Neurosurgery, Gangneung Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 2Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. dcsuh@amc.seoul.kr
- 3Department of Radiology, Soonchunhyang University Bucheon Hospital, Gyeonggi-do, Korea.
- 4Department of Radiology, Gyeongsang National University School of Medicine and Gyeongsang National University Changwon Hospital, Changwon, Korea.
- KMID: 2424049
- DOI: http://doi.org/10.5469/neuroint.2018.13.1.48
Abstract
- PURPOSE
False positive diagnoses of cerebral aneurysm via magnetic resonance angiography (MRA) screening may increase unnecessary cerebral catheter angiography. The purpose of this study was to investigate the effects of medical liability on medical decision-making during radiologic interpretation.
MATERIALS AND METHODS
We included 56 consecutive patients who were referred with suspected aneurysm based on MRA or computed tomography angiography (CTA) and showed no aneurysm on subsequent digital subtraction angiography (DSA). MRA and CTA were reviewed twice by two neuroradiology fellows who were blind as to whether the suspected lesions were true aneurysms or not. The second review was repeated after proposing that their decision was subject to legal liability and they would be responsible for medico-legal problems related to their diagnoses. Diagnostic differences based on each review were analyzed, focusing on changes in false positive diagnosis rates.
RESULTS
A total of 63 suspected aneurysmal lesions detected via MRA or CTA were found to be negative based on DSA. At first review, 32 lesions were diagnosed as true aneurysms by observer 1 and 27 by observer 2, corresponding to false positive rates of 51% and 43% respectively. At the second review, 39 lesions (62%) were diagnosed by observer 1, and 30 (48%) by observer 2. Thus, there was an overall increase in false positive aneurysm diagnosis of 11% for observer 1 and 5% for observer 2, after emphasizing their responsibilities in the context of medical litigation.
CONCLUSION
Concerns about medical liability could result in increased false positive diagnoses of cerebral aneurysms via MRA screening. Whether repeated follow-up of the suspected lesion or catheter angiographic confirmation is better with regard to long-term patient outcomes requires further study.
Keyword
MeSH Terms
Figure
-

Fig. 1 False positive diagnosis of an aneurysm (arrows) in the right A1. (A) An aneurysm was suggested in the right A1 on 3D-TOF MRA. (B) There was no definite aneurysm on cerebral angiogram. (C) Three dimensional angiogram showed a mild dilatation of the proximal A1. There was neither abnormal vessel wall thickness (D) nor abnormal enhancement (E) on vessel wall MRI.
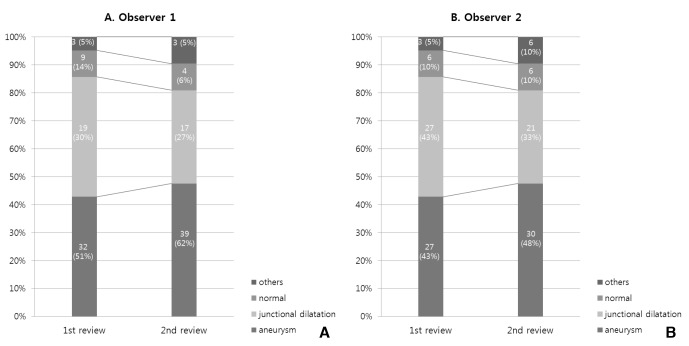
Fig. 2 Changes in diagnostic results from observer 1 (A) and observer 2 (B). Note increased false positive diagnosis rates of aneurysm after emphasizing the possibility of medical litigation (2nd review) in both observers
Reference
-
1. Pinto A, Brunese L, Pinto F, Reali R, Daniele S, Romano L. The concept of error and malpractice in radiology. Semin Ultrasound CT MR. 2012; 33:275–279. PMID: 22824117.
Article2. Brady AP. Error and discrepancy in radiology: Inevitable or avoidable? Insights Imaging. 2017; 8:171–182. PMID: 27928712.
Article3. Fileni A, Magnavita N, Mirk P, Iavicoli I, Magnavita G, Bergamaschi A. Radiologic malpractice litigation risk in italy: An observational study over a 14-year period. AJR Am J Roentgenol. 2010; 194:1040–1046. PMID: 20308508.
Article4. Villablanca JP, Jahan R, Hooshi P, Lim S, Duckwiler G, Patel A, et al. Detection and characterization of very small cerebral aneurysms by using 2d and 3d helical ct angiography. AJNR Am J Neuroradiol. 2002; 23:1187–1198. PMID: 12169479.5. Fischer S, Hopf N, Henkes H. Evolution from an infundibulum of the posterior communicating artery to a saccular aneurysm. Clin Neuroradiol. 2011; 21:87–90. PMID: 21140127.
Article6. Satoh T, Omi M, Ohsako C, Fujiwara K, Tsuno K, Sasahara W, et al. Differential diagnosis of the infundibular dilation and aneurysm of internal carotid artery: Assessment with fusion imaging of 3d mr cisternography/angiography. AJNR Am J Neuroradiol. 2006; 27:306–312. PMID: 16484398.7. Germino JC, Elmore JG, Carlos RC, Lee CI. Imaging-based screening: Maximizing benefits and minimizing harms. Clinical imaging. 2016; 40:339–343. PMID: 26112898.
Article8. Lee CS, Nagy PG, Weaver SJ, Newman-Toker DE. Cognitive and system factors contributing to diagnostic errors in radiology. AJR Am J Roentgenol. 2013; 201:611–617. PMID: 23971454.
Article9. Nahed BV, Babu MA, Smith TR, Heary RF. Malpractice liability and defensive medicine: A national survey of neurosurgeons. PLoS One. 2012; 7:e39237. PMID: 22761745.
Article10. Magnavita N, Fileni A, Mirk P, Magnavita G, Ricci S, Cotroneo AR. Malpractice claims in interventional radiology: Frequency, characteristics and protective measures. Radiol Med. 2013; 118:504–517. PMID: 22986698.
Article11. Mavroforou A, Giannoukas A, Mavrophoros D, Michalodimitrakis E. Physicians' liability in interventional radiology and endovascular therapy. Eur J Radiol. 2003; 46:240–243. PMID: 12758118.
Article12. Studdert DM, Mello MM, Sage WM, DesRoches CM, Peugh J, Zapert K, et al. Defensive medicine among high-risk specialist physicians in a volatile malpractice environment. JAMA. 2005; 293:2609–2617. PMID: 15928282.
Article13. Keedy A. An overview of intracranial aneurysms. Mcgill J Med. 2006; 9:141–146.
Article14. Adams WM, Laitt RD, Jackson A. The role of mr angiography in the pretreatment assessment of intracranial aneurysms: A comparative study. AJNR Am J Neuroradiol. 2000; 21:1618–1628. PMID: 11039340.15. Hoh BL, Cheung AC, Rabinov JD, Pryor JC, Carter BS, Ogilvy CS. Results of a prospective protocol of computed tomographic angiography in place of catheter angiography as the only diagnostic and pretreatment planning study for cerebral aneurysms by a combined neurovascular team. Neurosurgery. 2004; 54:1329–1340. discussion 1340-1322. PMID: 15157289.
Article16. Mallouhi A, Felber S, Chemelli A, Dessl A, Auer A, Schocke M, et al. Detection and characterization of intracranial aneurysms with mr angiography: Comparison of volume-rendering and maximum-intensity-projection algorithms. AJR Am J Roentgenol. 2003; 180:55–64. PMID: 12490476.
Article17. Sailer AM, Wagemans BA, Nelemans PJ, de Graaf R, van Zwam WH. Diagnosing intracranial aneurysms with mr angiography: Systematic review and meta-analysis. Stroke. 2014; 45:119–126. PMID: 24326447.18. Okuyama T, Saito K, Hirano A, Takahashi A, Hashimoto Y, Inagaki T. Diagnosis of unruptured cerebral aneurysms using magnetic resonance angiography and three dimensional computed tomographic angiography. No Shinkei Geka. 1997; 25:1073–1079. PMID: 9430141.19. Hiratsuka Y, Miki H, Kiriyama I, Kikuchi K, Takahashi S, Matsubara I, et al. Diagnosis of unruptured intracranial aneurysms: 3t mr angiography versus 64-channel multi-detector row ct angiography. Magn Reson Med Sci. 2008; 7:169–178. PMID: 19110511.
Article20. Wardlaw JM, White PM. The detection and management of unruptured intracranial aneurysms. Brain. 2000; 123(Pt 2):205–221. PMID: 10648430.
Article21. Kaufmann TJ, Huston J 3rd, Mandrekar JN, Schleck CD, Thielen KR, Kallmes DF. Complications of diagnostic cerebral angiography: Evaluation of 19,826 consecutive patients. Radiology. 2007; 243:812–819. PMID: 17517935.22. McKinney AM, Palmer CS, Truwit CL, Karagulle A, Teksam M. Detection of aneurysms by 64-section multidetector ct angiography in patients acutely suspected of having an intracranial aneurysm and comparison with digital subtraction and 3d rotational angiography. AJNR Am J Neuroradiol. 2008; 29:594–602. PMID: 18065510.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- False-positive Intracranial Aneurysms on MR Angiography: Incidence and Causes
- Analysis of Initial Angiographic False Negative Aneurysmal Patients and False Positive Non-Aneurysmal Patients
- Traumatic Aneurysm of Peripheral Cerebral Artery: A Case Report
- Imaging Features of Intracranial Calcified Aneurysm: Report of 4 Cases
- Distal Middle Cerebral Artery M4 Aneurysm Surgery Using Navigation-CT Angiography
