Chonnam Med J.
2018 Sep;54(3):190-196. 10.4068/cmj.2018.54.3.190.
Predictors of Clinical Outcome in Patients with Angiographically Intermediate Lesions with Minimum Lumen Area Less than 4 mm² Using Intravascular Ultrasound in Non-Proximal Epicardial Coronary Artery
- Affiliations
-
- 1Division of Cardiology, Chonnam National University Hospital, Cardiovascular Convergence Research Center Nominated by Korea Ministry of Health and Welfare, Gwangju, Korea. hyj200@hanmail.net
- KMID: 2420888
- DOI: http://doi.org/10.4068/cmj.2018.54.3.190
Abstract
- We investigated predictors of major adverse cardiac events (MACE) with two years after medical treatment for lesions with angiographically intermediate lesions with intravascular ultrasound (IVUS) minimum lumen area (MLA) <4 mm² in non-proximal epicardial coronary artery. We retrospectively enrolled 104 patients (57 males, 62±10 years) with angiographically intermediate lesions (diameter stenosis 30-70%) with IVUS MLA <4 mm² in the non-proximal epicardial coronary artery with a reference lumen diameter between 2.25 and 3.0 mm. We evaluated the incidences of major adverse cardiovascular events (MACE including death, myocardial infarction, target lesion and target vessel revascularizations, and cerebrovascular accident) two years after medical therapy. During the two-year follow-up, 15 MACEs (14.4%) (including 1 death, 2 myocardial infarctions, 10 target vessel revascularizations, and 2 cerebrovascular accidents) occurred. Diabetes mellitus was more prevalent (46.7% vs. 18.0%, p=0.013) and statins were used less frequently in patients with MACE compared with those without MACE (40.0% vs. 71.9%, p=0.015). Independent predictors of MACEs with two years included diabetes mellitus (odds ratio [OR]=3.41; 95% CI=1.43-8.39, p=0.020) and non-statin therapy (OR=3.11; 95% CI=1.14-6.50, p=0.027). Long-term event rates are relatively low with only medical therapy without any intervention, so the cut-off of IVUS MLA 4 mm² might be too large to be applied for defining significant stenosis. The predictors of long-term MACE were diabetes mellitus and statin therapy in patients with angiographically intermediate lesions in non-proximal epicardial coronary artery.
MeSH Terms
Figure
-
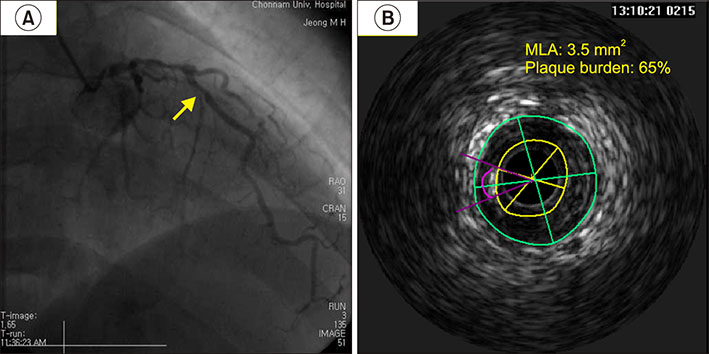
FIG. 1 Coronary angiographic (A) and intravascular ultrasound images (B) of angiographically intermediate lesions with intravascular ultrasound minimal lumen area (MLA) <4 mm2 in middle left anterior descending artery.
Reference
-
1. Abizaid A, Mintz GS, Pichard AD, Kent KM, Satler LF, Walsh CL, et al. Clinical, intravascular ultrasound, and quantitative angiographic determinants of the coronary flow reserve before and after percutaneous transluminal coronary angioplasty. Am J Cardiol. 1998; 82:423–428.
Article2. Nishioka T, Amanullah AM, Luo H, Berglund H, Kim CJ, Nagai T, et al. Clinical validation of intravascular ultrasound imaging for assessment of coronary stenosis severity: comparison with stress myocardial perfusion imaging. J Am Coll Cardiol. 1999; 33:1870–1878.
Article3. Briguori C, Anzuini A, Airoldi F, Gimelli G, Nishida T, Adamian M, et al. Intravascular ultrasound criteria for the assessment of the functional significance of intermediate coronary artery stenoses and comparison with fractional flow reserve. Am J Cardiol. 2001; 87:136–141.
Article4. Dhawan J, Bray CL. Are Asian coronary arteries smaller than caucasian? A study on angiographic coronary artery size estimation during life. Int J Cardiol. 1995; 49:267–269.
Article5. Lip GY, Rathore VS, Katira R, Watson RD, Singh SP. Do Indo-Asians have smaller coronary arteries. Postgrad Med J. 1999; 75:463–466.
Article6. Roberts WL, Moulton L, Law TC, Farrow G, Cooper-Anderson M, Savory J, et al. Evaluation of nine automated high-sensitivity C-reactive protein methods: implications for clinical and epidemiological applications. Part 2. Clin Chem. 2001; 47:418–425.
Article7. TIMI IIIB Investigators. Effects of tissue plasminogen activator and a comparison of early invasive and conservative strategies in unstable angina and non-Q-wave myocardial infarction. Results of the TIMI IIIB trial. Thrombolysis in myocardial ischemia. Circulation. 1994; 89:1545–1556.8. Mintz GS, Nissen SE, Anderson WD, Bailey SR, Erbel R, Fitzgerald PJ, et al. American college of cardiology clinical expert consensus document on standards for acquisition, measurement and reporting of intravascular ultrasound studies (IVUS): a report of the American college of cardiology task force on clinical expert consensus documents. J Am Coll Cardiol. 2001; 37:1478–1492.
Article9. Nakamura M, Nishikawa H, Mukai S, Setsuda M, Nakajima K, Tamada H, et al. Impact of coronary artery remodeling on clinical presentation of coronary artery disease: an intravascular ultrasound study. J Am Coll Cardiol. 2001; 37:63–69.
Article10. Stone GW, Maehara A, Lansky AJ, de Bruyne B, Cristea E, Mintz GS, et al. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011; 364:226–235.
Article11. Bech GJ, de Bruyne B, Pijls NH, de Muinck ED, Hoorntje JC, Escaned J, et al. Fractional flow reserve to determine the appropriateness of angioplasty in moderate coronary stenosis: a randomized trial. Circulation. 2001; 103:2928–2934.
Article12. Boyle PJ. Diabetes mellitus and macrovascular disease: mechanisms and mediators. Am J Med. 2007; 120:9 Suppl 2. S12–S17.
Article13. Stancoven A, McGuire DK. Preventing macrovascular complications in type 2 diabetes mellitus: glucose control and beyond. Am J Cardiol. 2007; 99:5H–11H.
Article14. Nicholls SJ, Tuzcu EM, Kalidindi S, Wolski K, Moon KW, Sipahi I, et al. Effect of diabetes on progression of coronary atherosclerosis and arterial remodeling: a pooled analysis of 5 intravascular ultrasound trials. J Am Coll Cardiol. 2008; 52:255–262.
Article15. Nissen SE, Tuzcu EM, Schoenhagen P, Crowe T, Sasiela WJ, Tsai J, et al. Reversal of Atherosclerosis with Aggressive Lipid Lowering (REVERSAL) Investigators. Statin therapy, LDL cholesterol, C-reactive protein, and coronary artery disease. N Engl J Med. 2005; 352:29–38.
Article16. Nissen SE, Nicholls SJ, Sipahi I, Libby P, Raichlen JS, Ballantyne CM, et al. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA. 2006; 295:1556–1565.
Article17. Nicholls SJ, Tuzcu EM, Sipahi I, Grasso AW, Schoenhagen P, Hu T, et al. Statins, high-density lipoprotein cholesterol, and regression of coronary atherosclerosis. JAMA. 2007; 297:499–508.
Article18. Kang SJ, Lee JY, Ahn JM, Mintz GS, Kim WJ, Park DW, et al. Validation of intravascular ultrasound-derived parameters with fractional flow reserve for assessment of coronary stenosis severity. Circ Cardiovasc Interv. 2011; 4:65–71.
Article19. Nam CW, Yoon HJ, Cho YK, Park HS, Kim H, Hur SH, et al. Outcomes of percutaneous coronary intervention in intermediate coronary artery disease: fractional flow reserve-guided versus intravascular ultrasound-guided. JACC Cardiovasc Interv. 2010; 3:812–817.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Predictors of Angiographic Restenosis after Intracoronary Stenting according to Stent Lumen Cross Sectional Area and Stent Length in Native Coronary Artery Lesions: An Intravascular Ultrasound Study
- PCI Optimization Using Intravascular Imaging: Insights From Recent Trials
- Efficacy of Interavascular Ultrasound in the Palmaz-Schatz Stent Implantation: Clinical Experience of 3 Coronary Artery Disease Patients
- Intravascular Ultrasound Findings of Coronary Wall Morphology in a Child with Kawasaki Disease
- Intravascular Ultrasound Findings of Arterial Remodeling at the Sites of Focal Coronary Spasm in Patients with Vasospatic Angina
