Deep Vein Thrombosis Due to Compression of Huge Hepatic Cyst Successfully Treated by Inferior Vena Cava Filter and Cyst Drainage
- Affiliations
-
- 1Department of Internal Medicine, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. nyheo@hanmail.net
- 2Department of Radiology, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2420753
- DOI: http://doi.org/10.4166/kjg.2018.72.3.146
Abstract
- An 88-year-old woman complained of right quadrant abdominal pain and severe edema in both legs. She had a history of pulmonary embolism one month ago. Abdomen CT showed a huge hepatic cyst compressing the intrahepatic portion of the inferior vena cava (IVC). The venogram CT showed multifocal thrombosis in the iliocaval and both lower extremity veins. Percutaneous hepatic cyst drainage was carried out. Fluid analysis presented leukocytosis, which suggested an infected hepatic cyst. To prevent secondary pulmonary thromboembolism, an IVC filter was inserted before catheter drainage for the hepatic cyst. One week later, abdominal pain was relieved. Then, sclerotherapy for the remnant hepatic cyst was performed by ethanol. Follow-up CT showed an increased amount of thrombosis in the iliocaval and left calf vein, but the IVC filter prevented another thromboembolic event successfully. The patient started dabigatran, a new oral anticoagulant, and compression stockings were applied to both legs. After one month, no visible thrombosis in the pelvis or either extremity was detected in abdominal CT. This case suggests that a huge hepatic cyst, especially with infection, should be considered as a possible cause of deep vein thrombosis if no other risk factors for thromboembolism exist.
Keyword
MeSH Terms
-
Abdomen
Abdominal Pain
Aged, 80 and over
Catheters
Dabigatran
Drainage*
Edema
Ethanol
Extremities
Female
Follow-Up Studies
Humans
Leg
Leukocytosis
Liver
Lower Extremity
Pelvis
Pulmonary Embolism
Risk Factors
Sclerotherapy
Stockings, Compression
Thromboembolism
Thrombosis
Tomography, X-Ray Computed
Veins
Vena Cava Filters*
Vena Cava, Inferior*
Venous Thrombosis*
Dabigatran
Ethanol
Figure
-
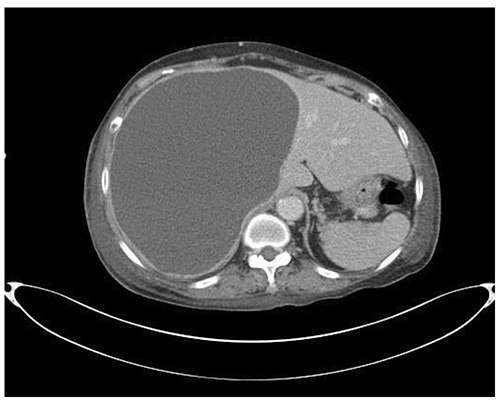
Fig. 1 Huge hepatic cyst compressing the intrahepatic portion of inferior vena cava was noted.

Fig. 2 Venogram extremity computed tomography showed thrombosis in the inferior vena cava below the renal vein (A, white arrow) and both femoral veins (B, white arrows) on the axial scan. A long segment of thrombosis near bifurcation of the inferior vena cava into common iliac veins was detected during the coronal scan (C, black arrows).
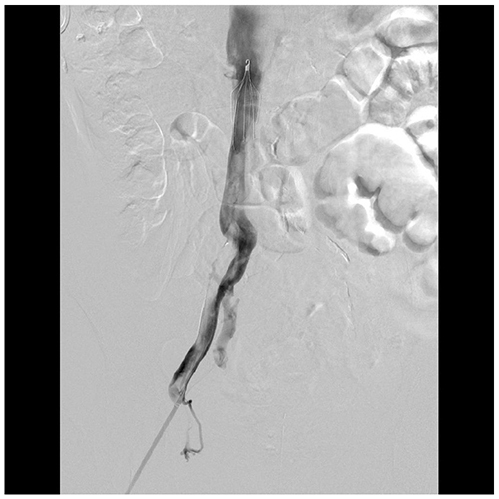
Fig. 3 Filter was inserted in the inferior vena cava, and filling defect due to thrombosis in the right common iliac vein was detected during venography.
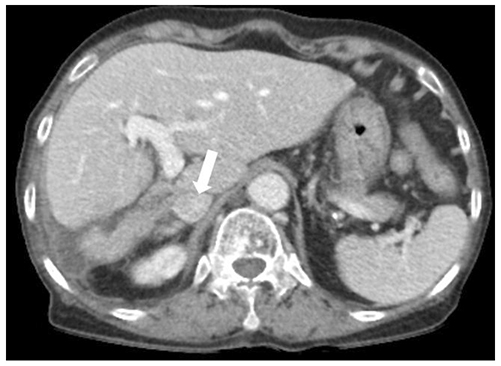
Fig. 4 Last follow-up CT at one month after cyst drainage and anticoagulation showed the patent inferior vena cava without thrombus (white arrow) and loss of hepatic cysts. CT, computed tomography.
Reference
-
1. Moon J, Heo D, Han S. A case of hepatic cyst-induced inferior vena cava thrombosis. Pak J Med Sci. 2014; 30:667–670.
Article2. Kashiwagi H, Kumagai K, Nozue M. Single incision laparoscopic surgery for a life-threatening, cyst of liver. Tokai J Exp Clin Med. 2011; 36:13–16.3. Musielak MC, Singh R, Hartman E, Bernstein J. Simple hepatic cyst causing inferior vena cava thrombus. Int J Surg Case Rep. 2014; 5:339–341.
Article4. England RA, Wells IP, Gutteridge CM. Benign external compression of the inferior vena cava associated with thrombus formation. Br J Radiol. 2005; 78:553–557.
Article5. Torzilli G, Santambrogio R, Vellini S, et al. Inferior vena cava thrombosis: an unusual complication of a large simple non-parasitic liver cyst requiring an integrated approach. Hepatogastroenterology. 2003; 50:2188–2191.6. Di Bisceglie AM, Befeler AS. Hepatic tumors and cysts. In : Feldman M, Friedman LS, Brandt LJ, editors. Sleisenger and fordtran's gastrointestinal and liver disease. 10th ed. Philadelphia: Saunder;2016. p. 1603–1627.7. Macedo FI. Current management of noninfectious hepatic cystic lesions: a review of the literature. World J Hepatol. 2013; 5:462–469.
Article8. Koperna T, Vogl S, Satzinger U, Schulz F. Nonparasitic cysts of the liver: results and options of surgical treatment. World J Surg. 1997; 21:850–854. discussion 854-855.
Article9. Cheng D, Amin P, Ha TV. Percutaneous sclerotherapy of cystic lesions. Semin Intervent Radiol. 2012; 29:295–300.
Article10. Moorthy K, Mihssin N, Houghton PW. The management of simple hepatic cysts: sclerotherapy or laparoscopic fenestration. Ann R Coll Surg Engl. 2001; 83:409–414.11. Bagot CN, Arya R. Virchow and his triad: a question of attribution. Br J Haematol. 2008; 143:180–190.
Article12. Leung TK, Lee CM, Chen HC. Fatal thrombotic complications of hepatic cystic compression of the inferior vena: a case report. World J Gastroenterol. 2005; 11:1728–1729.
Article13. Long J, Vaughan-Williams H, Moorhouse J, Sethi H, Kumar N. Acute Budd-Chiari syndrome due to a simple liver cyst. Ann R Coll Surg Engl. 2014; 96:109E–111E.
Article14. Iguchi S, Kasai A, Kishimoto H, et al. Thrombosis in inferior vena cava (IVC) due to intra-cystic hemorrhage into a hepatic local cyst with autosomal dominant polycystic kidney disease (ADPKD). Intern Med. 2004; 43:209–212.
Article15. Peces R, Gil F, Costero O, Pobes A. Massive inferior vena cava thrombosis in a patient with autosomal dominant polycystic hepatorenal disease. Nefrologia. 2002; 22:75–78.16. Gruttadauria S, Luca A, Cintorino D, Doria C, Scott VL, Marino IR. Hepatic hydatid cyst causing thrombosis of the inferior vena cava and complicated by hemobilia: a multimodal sequential approach in the treatment. Dig Dis Sci. 2003; 48:358–364.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Tilting after Placement of the Gunther-Tulip Inferior Vena Caval Filter: A Case Report
- Prophylactic Placement of Titanium Greenfield Vena Cava Filter before Surgical Removal of the Huge Leiomyoma Uteri Associated with Deep Vein Thrombosis: A case report
- lilac Vein Thrombosis: A Case Report of Treatment with Inferior Vena Cava Filter, Urokinase and Vascular Stent
- Trapping of Massive Thrombus in an Inferior Vena Cava Filter: Treatment with Additional Filter Placement and Aspiration Thrombectomy
- Temporary Inferior Vena Cava Filter Placement in Patients withDeep Vein Thrombosis
