Morphologic Changes of Femoral Cam Lesion after Osteoplasty for Femoroacetabular Impingement
- Affiliations
-
- 1Department of Orthopedic Surgery, Soonchunhyang University Gumi Hospital, Gumi, Korea.
- 2Department of Orthopedic Surgery, Chungnam National University School of Medicine, Daejeon, Korea. dshwang@cnu.ac.kr
- 3Department of Orthopedic Surgery, Yanbian University Hospital, Yanji, China.
- KMID: 2419466
- DOI: http://doi.org/10.4055/jkoa.2018.53.4.307
Abstract
- PURPOSE
We evaluated the morphologic change of cam lesion of femoroacetabular impingement (FAI) using 3-dimensional computed tomography (3D-CT) at the minimum 2-year follow-up and estimated its relationship with clinical outcomes.
MATERIALS AND METHODS
Between February 2007 and March 2014, all patients who underwent hip arthroscopic femoroplasty under the impression of FAI were retrospectively evaluated. We selected patients who received 3D-CT and were followed-up for more than 2 years. We estimated the quantitative volume of femoroplasty, alpha angle and femoral head-neck offset using 3D-CT.
RESULTS
Thirty-two patients (37 cases) were selected in our study. The mean age was 31.2 years (16-69 years) and the mean follow-up duration was 47.3 months (26-119 months). The mean resection volume measured after femoroplasty using 3D-CT was 48.9 mm2 (13.2-106.4 mm2), and follow-up mean resection volume was 37.9 mm2 (7.83-90.37 mm2). A little bit of the mean volumatic overgrowth of the resection area between immediate postoperative and last follow-up was shown; however, there was no statistically significant difference in the mean values (p>0.05). The clinical outcomes showed a significant improvement during the perioperative and follow-up periods in all categories (p < 0.05).
CONCLUSION
There was no significant regrowth of cam lesion after femoroplasty for FAI at maximum 9 years. Moreover, in most cases, clinical outcomes were improved. This suggests that we were able to achieve good clinical outcomes without harmful anatomical regrowth of cam deformity using arthroscopic femoroplasty.
MeSH Terms
Figure
-
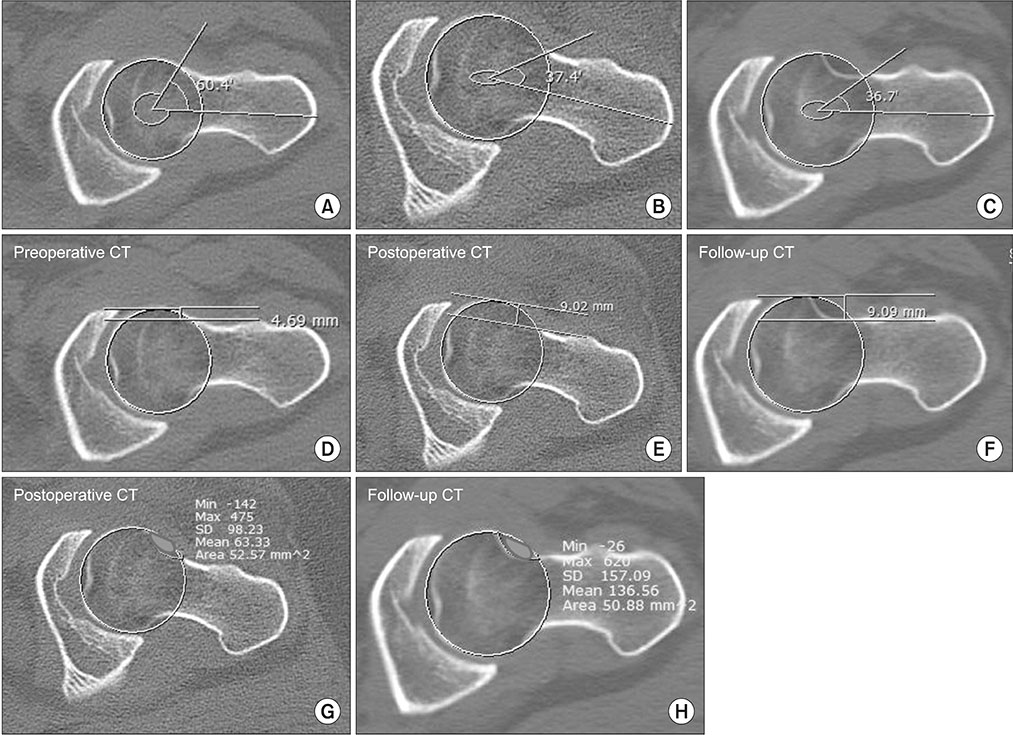
Figure 1 Computed tomography (CT) of pre- and postoperative and follow-up. Section of axial image was selected to measure the same level of resection area. (A) Preoperative alpha angle. (B) Postoperative alpha angle. (C) Follow-up alpha angle. (D) Preoperative femoral head-neck offset. (E) Postoperative femoral head-neck offset. (F) Follow-up femoral head-neck offset. (G) Resection area measurement of immediate postoperative CT. (H) Resection area measurement of follow CT.
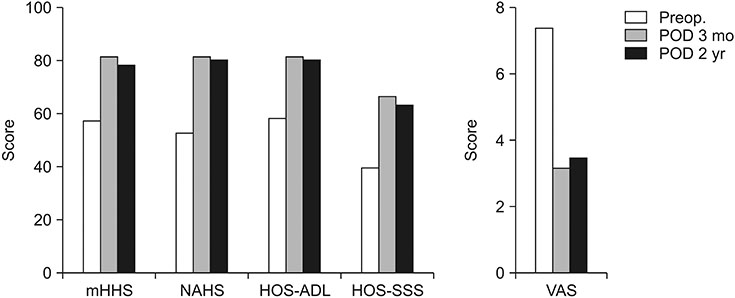
Figure 2 Clinical outcome score and pain score: preoperative (Preop.) and 2-month follow-up, and 2-year follow-up. POD, postoperative day; mHHS, modified Harris hip score; NAHS, non-arthritic hip score; HOS-ADL, hip outcome score-activities of daily living; HOS-SSS, hip outcome score-sport specific subscale; VAS, visual analogue scale.
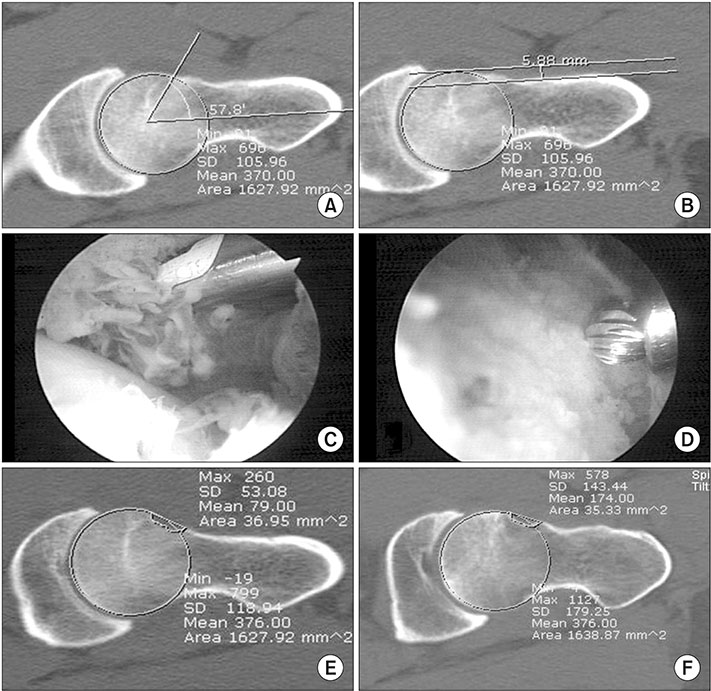
Figure 3 A 21-year-old male patient presented with right side anterior groin pain with positive anterior impingement test. Radiologic evaluation before the operation showed abnormal findings. Radiologic evaluation at 119 months, showed no regrowth at the previous resection area. (A) Preoperative alpha angle ('06. Aug.). (B) Preoperative femoral head-neck offset ('06. Aug.). (C, D) Intraoperative arthroscopic finding ('06. Aug.). (E) Postoperative computed tomography (CT) scan ('06. Aug.). (F) Following CT scan at 119 months after surgery ('16. Jul.).
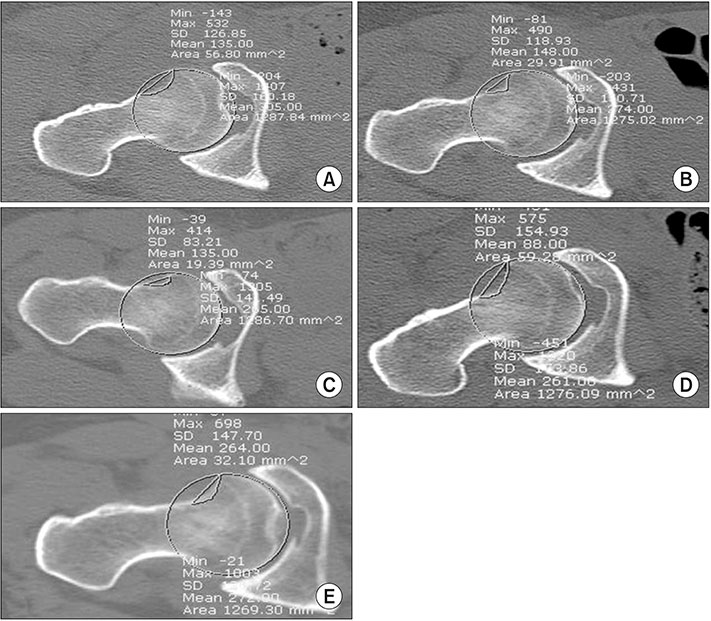
Figure 4 A 29-year-old female patient underwent the operation after the diagnosis of femoroacetabular impingement. (A) Arthroscopic femoral bumpectomy was performed. (B, C) During the follow-up period, she felt hip pain. Axial oblique computed tomography (CT) scan of hip at the follow-up revealed regrowth at the previous resection area. She underwent revision hip arthroscopy (D) and has had no further episodes of hip pain after revision surgery (E). (A) First operation: postoperative CT scan ('09 Sep.). (B) First operation: first follow-up (F/U) (postoperative day [POD] 11 months from first operation, '11 Sep.). (C) First operation: second F/U (POD 41 months from first operation, '12 Jul.). (D) Second operation: postoperative CT scan ('12 Jul.). (E) Second operation: third F/U (POD 49 months from second operation, '16 Aug.).
Reference
-
1. Byrd JW. Hip arthroscopy: patient assessment and indications. Instr Course Lect. 2003; 52:711–719.2. Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003; 417:112–120.3. Smith-Petersen MN. The classic: treatment of malum coxae senilis, old slipped upper femoral epiphysis, intrapelvic protrusion of the acetabulum, and coxa plana by means of acetabuloplasty. 1936. Clin Orthop Relat Res. 2009; 467:608–615.4. Ito K, Minka MA 2nd, Leunig M, Werlen S, Ganz R. Femoroacetabular impingement and the cam-effect. A MRI-based quantitative anatomical study of the femoral head-neck offset. J Bone Joint Surg Br. 2001; 83:171–176.5. Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002; 84:556–560.
Article6. Reynolds D, Lucas J, Klaue K. Retroversion of the acetabulum. A cause of hip pain. J Bone Joint Surg Br. 1999; 81:281–288.7. Siebenrock KA, Schoeniger R, Ganz R. Anterior femoro-acetabular impingement due to acetabular retroversion. Treatment with periacetabular osteotomy. J Bone Joint Surg Am. 2003; 85:278–286.8. Anderson LA, Peters CL, Park BB, Stoddard GJ, Erickson JA, Crim JR. Acetabular cartilage delamination in femoroacetabular impingement. Risk factors and magnetic resonance imaging diagnosis. J Bone Joint Surg Am. 2009; 91:305–313.9. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005; 87:1012–1018.10. Wagner S, Hofstetter W, Chiquet M, et al. Early osteoarthritic changes of human femoral head cartilage subsequent to femoro-acetabular impingement. Osteoarthritis Cartilage. 2003; 11:508–518.
Article11. Siebenrock KA, Wahab KH, Werlen S, Kalhor M, Leunig M, Ganz R. Abnormal extension of the femoral head epiphysis as a cause of cam impingement. Clin Orthop Relat Res. 2004; 418:54–60.
Article12. Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop Relat Res. 2004; 418:67–73.13. Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001; 83:1119–1124.14. Byrd JW. Hip arthroscopy by the supine approach. Instr Course Lect. 2006; 55:325–336.15. Philippon MJ, Schenker ML. Arthroscopy for the treatment of femoroacetabular impingement in the athlete. Clin Sports Med. 2006; 25:299–308. ix
Article16. Philippon MJ, Stubbs AJ, Schenker ML, Maxwell RB, Ganz R, Leunig M. Arthroscopic management of femoroacetabular impingement: osteoplasty technique and literature review. Am J Sports Med. 2007; 35:1571–1580.17. Byrd JW, Jones KS. Prospective analysis of hip arthroscopy with 2-year follow-up. Arthroscopy. 2000; 16:578–587.
Article18. Tannast M, Siebenrock KA. Conventional radiographs to assess femoroacetabular impingement. Instr Course Lect. 2009; 58:203–212.19. Philippon MJ, Schenker ML, Briggs KK, Kuppersmith DA, Maxwell RB, Stubbs AJ. Revision hip arthroscopy. Am J Sports Med. 2007; 35:1918–1921.
Article20. Gupta A, Redmond JM, Stake CE, Finch NA, Dunne KF, Domb BG. Does the femoral cam lesion regrow after osteoplasty for femoroacetabular impingement? Two-year follow-up. Am J Sports Med. 2014; 42:2149–2155.21. Byrd JW. Evaluation of the hip: history and physical examination. N Am J Sports Phys Ther. 2007; 2:231–240.22. Christensen CP, Althausen PL, Mittleman MA, Lee JA, McCarthy JC. The nonarthritic hip score: reliable and validated. Clin Orthop Relat Res. 2003; 406:75–83.
Article23. Leunig M, Ganz R. Femoroacetabular impingement. A common cause of hip complaints leading to arthrosis. Unfallchirurg. 2005; 108:9–10. 12–17.24. Byrd JW, Jones KS. Diagnostic accuracy of clinical assessment, magnetic resonance imaging, magnetic resonance arthrography, and intra-articular injection in hip arthroscopy patients. Am J Sports Med. 2004; 32:1668–1674.
Article25. Bardakos NV, Vasconcelos JC, Villar RN. Early outcome of hip arthroscopy for femoroacetabular impingement: the role of femoral osteoplasty in symptomatic improvement. J Bone Joint Surg Br. 2008; 90:1570–1575.26. Papalia R, Del Buono A, Franceschi F, Marinozzi A, Maffulli N, Denaro V. Femoroacetabular impingement syndrome management: arthroscopy or open surgery? Int Orthop. 2012; 36:903–914.
Article27. May DA, Snearly WN, Bents R, Jones R. MR imaging findings in anterior cruciate ligament reconstruction: evaluation of notchplasty. AJR Am J Roentgenol. 1997; 169:217–222.
Article28. Dudda M, Albers C, Mamisch TC, Werlen S, Beck M. Do normal radiographs exclude asphericity of the femoral headneck junction? Clin Orthop Relat Res. 2009; 467:651–659.
Article29. Heyworth BE, Shindle MK, Voos JE, Rudzki JR, Kelly BT. Radiologic and intraoperative findings in revision hip arthroscopy. Arthroscopy. 2007; 23:1295–1302.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Second-look Hip Arthroscopy after Arthroscopic Labrectomy of the Hip: Preliminary Report
- Arthroscopic Treatment of Cam Type Femoroacetabular Impingement: Short Term Results
- Prevalence of Cam Deformity with Associated Femoroacetabular Impingement Syndrome in Hip Joint Computed Tomography of Asymptomatic Adults
- Efficacy of Intra-articular Steroid Injection in Patients with Femoroacetabular Impingement
- Short-Term Results of Osteochondral Autologous Transfer and Femoral Neck Osteochondroplasty for the Treatment of Osteochondral Lesions of the Femoral Head and Concomitant Femoroacetabular Impingement Syndrome: A Case Series
