Prevalence of Cam Deformity with Associated Femoroacetabular Impingement Syndrome in Hip Joint Computed Tomography of Asymptomatic Adults
- Affiliations
-
- 1Department of Orthopaedic Surgery, Ajou University College of Medicine, Suwon, Korea. yeyeonwon@gmail.com
- 2Department of Orthopaedic, Cheil General Hospital and Women's Healthcare Center, Dankook University College of Medicine, Cheonan, Korea.
- KMID: 2408179
- DOI: http://doi.org/10.5371/hp.2018.30.1.5
Abstract
- PURPOSE
Femoroacetabular impingement (FAI) is considered an important cause of early degenerative arthritis development. Although three-dimensional (3D) imaging such as computed tomography (CT) and magnetic resonance imaging are considered precise imaging modalities for 3D morphology of FAI, they are associated with several limitations when used in out-patient clinics. The paucity of FAI morphologic data in Koreans makes it difficult to select the most effective radiographical method when screening for general orthopedic problems. We postulate that there might be an individual variation in the distribution of cam deformity in the asymptomatic Korean population.
MATERIALS AND METHODS
From January 2011 to December 2015, CT images of the hips of 100 subjects without any history of hip joint ailments were evaluated. A computer program which generates 3D models from CT scans was used to provide sectional images which cross the central axis of the femoral head and neck. Alpha angles were measured in each sectional images. Alpha angles above 55° were regarded as cam deformity.
RESULTS
The mean alpha angle was 43.5°, range 34.7-56.1°(3 o'clock); 51.24°, range 39.5-58.8°(2 o'clock); 52.45°, range 43.3-65.5°(1 o'clock); 44.09°, range 36.8-49.8°(12 o'clock); 40.71, range 33.5-45.8°(11 o'clock); and 39.21°, range 34.1-44.6°(10 o'clock). Alpha angle in 1 and 2 o'clock was significantly larger than other locations (P < 0.01). The prevalence of cam deformity was 18.0% and 19.0% in 1 and 2 o'clock, respectively.
CONCLUSION
Cam deformity of FAI was observed in 31% of asymptomatic hips. The most common region of cam deformity was antero-superior area of femoral head-neck junction (1 and 2 o'clock).
MeSH Terms
Figure
-
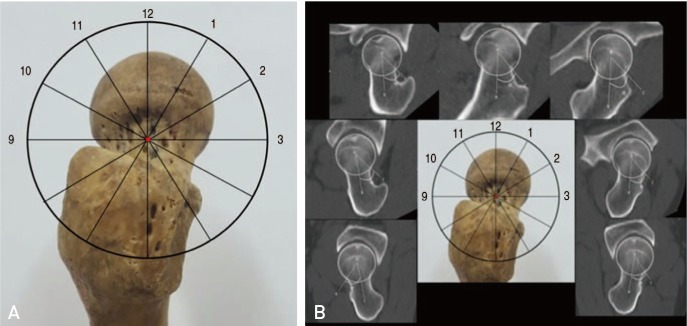
Fig. 1 (A) The 12 o'clock position was defined as the superior aspect of the proximal femur in a standing position. (B) The alpha angle was assessed from the line drawn between the center of the femoral neck at its narrowest point and the center of the femoral head at clock-face positions at 30°intervals using three-dimensional reconstruction of computed tomography imaging of the femur.

Fig. 2 Point A is the center of the femoral head and the line drawn from A to B is the long axis line connecting the centers between the femur head and neck. The line drawn from A to C is the line extending from the center of the femoral head to the point the femoral head extrudes a circle drawn around the femoral head. The angle formed between these two lines is defined as alpha. The alpha angle is described as the angle formed by the femoral neck axial line and the line from the center of the femoral head to a point where the femoral head extends outside the circle around the femoral head.
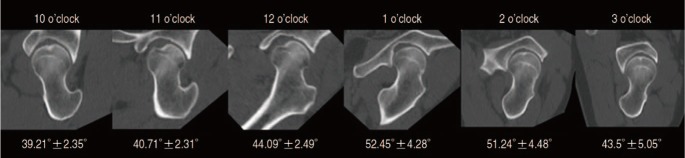
Fig. 3 Mean alpha angles of different clock-face positions.
Reference
-
1. Ganz R, Bamert P, Hausner P, Isler B, Vrevc F. [Cervico-acetabular impingement after femoral neck fracture]. Unfallchirurg. 1991; 94:172–175. German. PMID: 2063213.2. Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003; (417):112–120.3. Bardakos NV, Villar RN. Predictors of progression of osteoarthritis in femoroacetabular impingement: a radiological study with a minimum of ten years follow-up. J Bone Joint Surg Br. 2009; 91:162–169. PMID: 19190047.4. Kubiak-Langer M, Tannast M, Murphy SB, Siebenrock KA, Langlotz F. Range of motion in anterior femoroacetabular impingement. Clin Orthop Relat Res. 2007; 458:117–124. PMID: 17206102.
Article5. Anderson K, Strickland SM, Warren R. Hip and groin injuries in athletes. Am J Sports Med. 2001; 29:521–533. PMID: 11476397.
Article6. Siebenrock KA, Ferner F, Noble PC, Santore RF, Werlen S, Mamisch TC. The cam-type deformity of the proximal femur arises in childhood in response to vigorous sporting activity. Clin Orthop Relat Res. 2011; 469:3229–3240. PMID: 21761254.
Article7. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005; 87:1012–1018. PMID: 15972923.8. Leunig M, Ganz R. [Femoroacetabular impingement. A common cause of hip complaints leading to arthrosis]. Unfallchirurg. 2005; 108:9–10. 12–17. German. PMID: 15619064.9. Clohisy JC, St John LC, Schutz AL. Surgical treatment of femoroacetabular impingement: a systematic review of the literature. Clin Orthop Relat Res. 2010; 468:555–564. PMID: 19830504.
Article10. Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002; 84:556–560. PMID: 12043778.
Article11. Van Houcke J, Yau WP, Yan CH, et al. Prevalence of radiographic parameters predisposing to femoroacetabular impingement in young asymptomatic Chinese and white subjects. J Bone Joint Surg Am. 2015; 97:310–317. PMID: 25695983.
Article12. Rakhra KS, Sheikh AM, Allen D, Beaulé PE. Comparison of MRI alpha angle measurement planes in femoroacetabular impingement. Clin Orthop Relat Res. 2009; 467:660–665. PMID: 19037709.
Article13. Dudda M, Albers C, Mamisch TC, Werlen S, Beck M. Do normal radiographs exclude asphericity of the femoral head-neck junction? Clin Orthop Relat Res. 2009; 467:651–659. PMID: 19023635.
Article14. Ahn T, Kim CH, Kim TH, et al. What is the prevalence of radiographic hip findings associated with femoroacetabular impingement in asymptomatic Asian volunteers? Clin Orthop Relat Res. 2016; 474:2655–2661. PMID: 27506973.
Article15. Kim J, Choi JA, Lee E, Lee KR. Prevalence of imaging features on CT thought to be associated with femoroacetabular impingement: a retrospective analysis of 473 asymptomatic adult hip joints. AJR Am J Roentgenol. 2015; 205:W100–W105. PMID: 26102406.
Article16. Pfirrmann CW, Mengiardi B, Dora C, Kalberer F, Zanetti M, Hodler J. Cam and pincer femoroacetabular impingement: characteristic MR arthrographic findings in 50 patients. Radiology. 2006; 240:778–785. PMID: 16857978.
Article17. Neumann M, Cui Q, Siebenrock KA, Beck M. Impingement-free hip motion: the ‘normal’ angle alpha after osteochondroplasty. Clin Orthop Relat Res. 2009; 467:699–703. PMID: 19018605.
Article18. Fukushima K, Uchiyama K, Takahira N, et al. Prevalence of radiographic findings of femoroacetabular impingement in the Japanese population. J Orthop Surg Res. 2014; 9:25. PMID: 24725368.
Article19. Takeyama A, Naito M, Shiramizu K, Kiyama T. Prevalence of femoroacetabular impingement in Asian patients with osteoarthritis of the hip. Int Orthop. 2009; 33:1229–1232. PMID: 19277653.
Article20. Ito K, Minka MA 2nd, Leunig M, Werlen S, Ganz R. Femoroacetabular impingement and the cam-effect. A MRI-based quantitative anatomical study of the femoral head-neck offset. J Bone Joint Surg Br. 2001; 83:171–176. PMID: 11284559.21. Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, Leunig M. Anterior femoroacetabular impingement: part I. Techniques of joint preserving surgery. Clin Orthop Relat Res. 2004; (418):61–66.22. Hack K, Di Primio G, Rakhra K, Beaulé PE. Prevalence of cam-type femoroacetabular impingement morphology in asymptomatic volunteers. J Bone Joint Surg Am. 2010; 92:2436–2444. PMID: 20962194.
Article23. Sutter R, Dietrich TJ, Zingg PO, Pfirrmann CW. How useful is the alpha angle for discriminating between symptomatic patients with cam-type femoroacetabular impingement and asymptomatic volunteers? Radiology. 2012; 264:514–521. PMID: 22653190.
Article24. Siebenrock KA, Kaschka I, Frauchiger L, Werlen S, Schwab JM. Prevalence of cam-type deformity and hip pain in elite ice hockey players before and after the end of growth. Am J Sports Med. 2013; 41:2308–2313. PMID: 23911701.
Article25. Agricola R, Heijboer MP, Ginai AZ, et al. A cam deformity is gradually acquired during skeletal maturation in adolescent and young male soccer players: a prospective study with minimum 2-year follow-up. Am J Sports Med. 2014; 42:798–806. PMID: 24585362.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Femoroacetabular Impingement Syndrome
- Efficacy of Intra-articular Steroid Injection in Patients with Femoroacetabular Impingement
- Controversial Issues in Arthroscopic Surgery for Femoroacetabular Impingement
- Descriptive Epidemiology of Symptomatic Femoroacetabular Impingement in Young Athlete: Single Center Study
- Usefulness of Hip Joint AP Plain X-ray Radiographs in Femoroacetabular Impingement
