Tree-in-Bud Pattern of Pulmonary Tuberculosis on Thin-Section CT: Pathological Implications
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul 03080, Korea. imjgsnu@gmail.com
- 2Department of Radiology, Samsung Medical Center, Seoul 06351, Korea.
- 3University of Fukui, School of Medical Sciences, Bunkyo, Fukui-shi, Fukui 910-8507, Japan.
- KMID: 2418548
- DOI: http://doi.org/10.3348/kjr.2018.19.5.859
Abstract
- The "tree-in-bud-pattern" of images on thin-section lung CT is defined by centrilobular branching structures that resemble a budding tree. We investigated the pathological basis of the tree-in-bud lesion by reviewing the pathological specimens of bronchograms of normal lungs and contract radiographs of the post-mortem lungs manifesting active pulmonary tuberculosis. The tree portion corresponds to the intralobular inflammatory bronchiole, while the bud portion represents filling of inflammatory substances within alveolar ducts, which are larger than the corresponding bronchioles. Inflammatory bronchiole per se represents the "tree" (stem) and inflammatory alveolar ducts constitute the "buds" or clubbing. "Clusters of micronodules", seen on 7-mm thick post-mortem radiographs with tuberculosis proved to be clusters of tree-in-bud lesions within the three-dimensional space of secondary pulmonary lobule based on radiological/pathological correlation. None of the post-mortem lung specimens showed findings of lung parenchymal lymphatics involvement.
Keyword
Figure
-
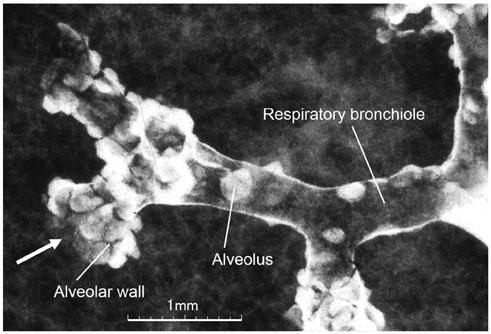
Fig. 1 Post-mortem bronchiologram. Respiratory bronchioles and central part of alveolar duct are demonstrated. Respiratory bronchioles are equipped with alveoli. Diameter of alveolar duct is larger than that of respiratory bronchiole, because diameter of alveoli is added to that of ductal lumen (arrow).
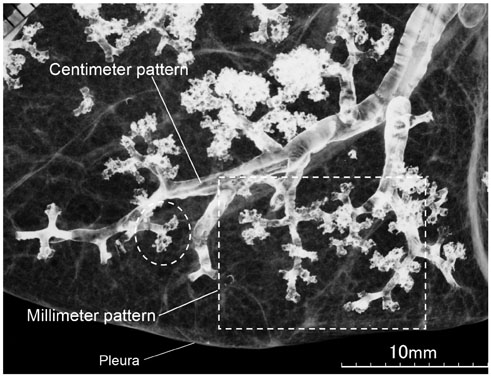
Fig. 2 Post-mortem bronchiologram. Two types of bronchiolar branching, cm and mm pattern, are demonstrated. Latter (boxed area) is morphological basis of tree-in-bud lesions in pulmonary tuberculosis. Extreme end of mm pattern is ballooned-out with fuzzy outline, which indicates alveolar ducts (circle).
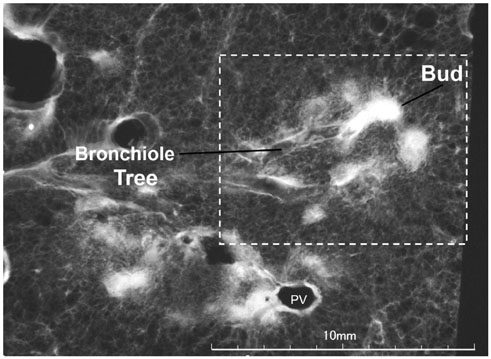
Fig. 3 Post-mortem radiograph of patient with active pulmonary tuberculosis demonstrating tree-in-bud lesion (boxed area) with smooth marginated bronchiole (tree) and distal clubbed end (bud). Bud measures 1–2 mm in diameter and is definitely bigger than parent bronchiole (tree). Slice thickness is 1 mm. PV = pulmonary vein
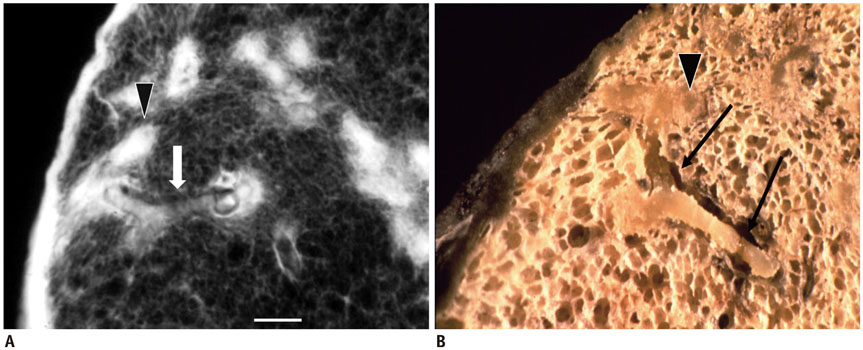
Fig. 4 Pathologic basis of tree-in-bud lesion. Post-mortem radiograph (A) and gross photograph (B) of same specimen in patient with pulmonary tuberculosis. Impacted cheesy material within smooth-marginated bronchiole (arrows) continues to larger, rather ill-defined alveolar ducts (arrowheads). Bar indicates 1 mm. Reprinted with permission from authors' reference 1. Adapted from Im et al. Radiology 1993;186:653-660
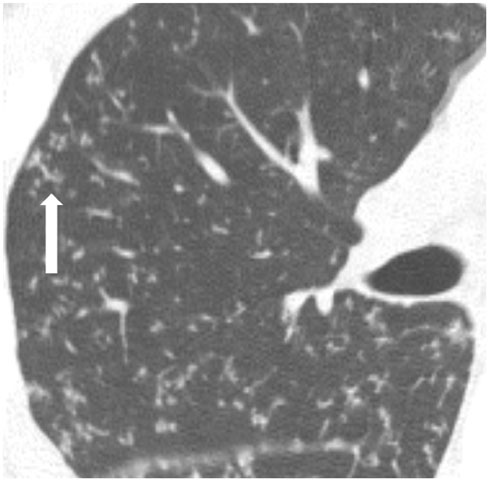
Fig. 5 CT image of tree-in-bud lesions in patient with active pulmonary tuberculosis. Note that tree ends in terminal clubbing (bud) (arrow). Note also that tree-in-bud lesions appear dense and well-defined even with small size; standard window setting (width 1600, level 250 HU).

Fig. 6 Comparison of centrilobular branching nodules seen in bacterial pneumonia (A) and tuberculosis (B). Note that marginal clarity of centrilobular nodules (arrows) are much greater in pulmonary tuberculosis (B) than in bacterial pneumonia (A).

Fig. 7 Post-mortem radiographs of cluster of micronodules (galaxy appearance described in sarcoidosis) and corresponding microscopic findings in patient with endobronchial spread of tuberculosis. A. Micronodules ≥ 2 mm are clustered within secondary pulmonary lobule, demarcated by interlobular septa (interrupted line) and PV. Bronchiole enters central portion of lobule (Br). PA indicates pulmonary artery. Bar indicates 10 mm; slice thickness is 7 mm. B. Serial thin-section radiographs reveal separation of each clustered nodule, with occasional continuity and branching. In lower right image, branching linear lesions occur predominantly at periphery of lobule abutting interlobular septa (arrowheads). If this plane were imaged by CT, it might have erroneously been interpreted as perilymphatic location. Bar indicates 5 mm; slice thickness is 1 mm. C. Close-up view of lower central section shows centrilobular patent bronchiole (Br) continuing into smooth marginated impacted bronchioles (tree), terminating in irregular marginated clubbed ends (buds). These findings suggest that cluster of small nodules observed on CT of patients with tuberculosis represent aggregates of tree-in-bud lesions. D. Pathologic specimen of same region shows central patent bronchiole, which continues into respiratory bronchiole with cheesy material; peripherally located cheesy material with inflammatory debris extending into surrounding alveoli (H&E, ×10).
Cited by 1 articles
-
Diagnosis of pulmonary tuberculosis
Byung Woo Jhun, Hee Jae Huh, Won-Jung Koh
J Korean Med Assoc. 2019;62(1):18-24. doi: 10.5124/jkma.2019.62.1.18.
Reference
-
1. Im JG, Itoh H, Shim YS, Lee JH, Ahn J, Han MC, et al. Pulmonary tuberculosis: CT findings--early active disease and sequential change with antituberculous therapy. Radiology. 1993; 186:653–660.
Article2. Collins J, Blankenbaker D, Stern EJ. CT patterns of bronchiolar disease: what is “tree-in-bud”. AJR Am J Roentgenol. 1998; 171:365–370.
Article3. Eisenhuber E. The tree-in-bud sign. Radiology. 2002; 222:771–772.
Article4. Rossi SE, Franquet T, Volpacchio M, Giménez A, Aguilar G. Tree-in-bud pattern at thin-section CT of the lungs: radiologic-pathologic overview. Radiographics. 2005; 25:789–801.
Article5. Gosset N, Bankier AA, Eisenberg RL. Tree-in-bud pattern. AJR Am J Roentgenol. 2009; 193:W472–W477.
Article6. Verma N, Chung JH, Mohammed TL. “Tree-in-bud sign”. J Thorac Imaging. 2012; 27:W27.
Article7. Li Q, Fan X, Huang XT, Luo TY, Chu ZG, Chen L, et al. Tree-in-bud pattern in central lung cancer: CT findings and pathologic correlation. Lung Cancer. 2015; 88:260–266.
Article8. Tack D, Nollevaux MC, Gevenois PA. Tree-in-bud pattern in neoplastic pulmonary emboli. AJR Am J Roentgenol. 2001; 176:1421–1422.
Article9. Franquet T, Giménez A, Prats R, Rodríguez-Arias JM, Rodríguez C. Thrombotic microangiopathy of pulmonary tumors: a vascular cause of tree-in-bud pattern on CT. AJR Am J Roentgenol. 2002; 179:897–899.
Article10. Li Ng Y, Hwang D, Patsios D, Weisbrod G. Tree-in-bud pattern on thoracic CT due to pulmonary intravascular metastases from pancreatic adenocarcinoma. J Thorac Imaging. 2009; 24:150–151.
Article11. Moon JW, Lee HY, Han J, Lee KS. Tree-in-bud sign as a manifestation of localized pulmonary lymphatic metastasis from a pancreas cancer. Intern Med. 2011; 50:3027–3029.12. Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008; 246:697–722.
Article13. Heo JN, Choi YW, Jeon SC, Park CK. Pulmonary tuberculosis: another disease showing clusters of small nodules. AJR Am J Roentgenol. 2005; 184:639–642.
Article14. Ko JM, Park HJ, Kim CH. Clinicoradiologic evidence of pulmonary lymphatic spread in adult patients with tuberculosis. AJR Am J Roentgenol. 2015; 204:38–43.
Article15. Heitzman ER. The lung: radiologic pathologic correlations. 2nd ed. St Louis, MO: Mosby;1984. p. 4–9.16. Itoh H, Tokunaga S, Asamoto H, Furuta M, Funamoto Y, Kitaichi M, et al. Radiologic-pathologic correlations of small lung nodules with special reference to peribronchiolar nodules. AJR Am J Roentgenol. 1978; 130:223–231.
Article17. Reid L, Simon G. The peripheral pattern in the normal bronchogram and its relation to peripheral pulmonary anatomy. Thorax. 1958; 13:103–109.
Article18. Hunter RL. Pathology of post primary tuberculosis of the lung: an illustrated critical review. Tuberculosis (Edinb). 2011; 91:497–509.
Article19. Akira M, Kitatani F, Lee YS, Kita N, Yamamoto S, Higashihara T, et al. Diffuse panbronchiolitis: evaluation with high-resolution CT. Radiology. 1988; 168:433–438.
Article20. Nakatsu M, Hatabu H, Morikawa K, Uematsu H, Ohno Y, Nishimura K, et al. Large coalescent parenchymal nodules in pulmonary sarcoidosis: “sarcoid galaxy” sign. AJR Am J Roentgenol. 2002; 178:1389–1393.
Article21. Mays TJ. Pulmonary consumption, pneumonia, and allied diseases of the lungs: their etiology, pathology and treatment, with a chapter on physical diagnosis. 1st ed. New York, NY: E.B. Treat & Co.;1901. p. 247–288.22. Gunn FD. Tuberculosis. In : Anderson WAD, editor. Pathology. 4th ed. St Louis, MO: C.V. Mosby Company;1961. p. 246–263.23. Haque AK. The pathology and pathophysiology of mycobacterial infections. J Thorac Imaging. 1990; 5:8–16.
Article24. Basaraba RJ, Smith EE, Shanley CA, Orme IM. Pulmonary lymphatics are primary sites of Mycobacterium tuberculosis infection in guinea pigs infected by aerosol. Infect Immun. 2006; 74:5397–5401.25. Kim WS, Choi JI, Cheon JE, Kim IO, Yeon KM, Lee HJ. Pulmonary tuberculosis in infants: radiographic and CT findings. AJR Am J Roentgenol. 2006; 187:1024–1033.
Article26. Kim WS, Moon WK, Kim IO, Lee HJ, Im JG, Yeon KM, et al. Pulmonary tuberculosis in children: evaluation with CT. AJR Am J Roentgenol. 1997; 168:1005–1009.
Article27. Miller WT Jr, Panosian JS. Causes and imaging patterns of tree-in-bud opacities. Chest. 2013; 144:1883–1892.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Thin-Section CT Findings of Nontuberculous Mycobacterial Pulmonary Diseases: Comparison Between Mycobacterium avium-intracellulare Complex and Mycobacterium abscessus Infection
- Pulmonary Manifestations of Fat Embolism on Thin-section CT: A Case Report
- Pulmonary Tuberculosis with Airspace Consolidation vs Mycoplasma Pneumonia in Adults: High-Resolution CT Findings
- Cystic Lung Changes in a Thin Section CT in an Asymptomatic Young Adult with Unilateral Pulmonary Vein Atresia: A Case Report
- Hematogenous Candida Pneumonia in Major Burn Patients: Plain Chest Radiograph and Thin-section CT Findings
