Intracranial Mirror Aneurysms: Anatomic Characteristics and Treatment Options
- Affiliations
-
- 1Department of Neurosurgery, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul 06974, Korea.
- 2Department of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul 03080, Korea. aronnn@naver.com
- 3Department of Neurosurgery, Dongguk University Ilsan Hospital, Dongguk University College of Medicine, Goyang 10326, Korea.
- 4Department of Neurosurgery, Kwangju Christian Hospital, Gwangju 61661, Korea.
- 5Department of Neurology, International St. Mary's Hospital, Catholic Kwandong University of Korea College of Medicine, Incheon 22711, Korea.
- 6Department of Neurosurgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul 03080, Korea.
- KMID: 2418547
- DOI: http://doi.org/10.3348/kjr.2018.19.5.849
Abstract
OBJECTIVE
Mirror aneurysms are generally considered as a subset of multiple aneurysms, defined as aneurysms occurring bilaterally and symmetrically on the same-named vessels. Although not infrequent, the characteristics of mirror aneurysms are not well studied. This investigation was conducted to elucidate the anatomic features of such lesions and examine treatment options.
MATERIALS AND METHODS
A retrospective review was conducted, aimed at 172 patients treated for 344 mirror aneurysms between January 2007 and December 2015. Aneurysms of similar nature but in asymmetric locations on the same-named vessels were excluded. All available records were examined and lesion characteristics, as well as treatment outcomes were assessed.
RESULTS
In study subjects (n = 172), mirror aneurysms most often involved middle cerebral artery bifurcation (n = 83), followed by a paraclinoid internal carotid artery (n = 50) and posterior communicating artery (n = 21). Most of the lesions (95.3%) measured ≤ 10 mm, and in 126 patients (74.6%), the size ratios were > 50%. Of the 344 aneurysms studied, coil embolization was undertaken in 217, surgical clipping in 62, and observation alone (no treatment) in 65. Coil embolization and surgical clipping were done bilaterally in 83 and 12 patients, respectively. In 12 patients, combined coiling and clipping were implemented on each side. Single-stage coil embolization of both the aneurysms was performed in 73 patients, with excellent post-procedural (85.6%) and follow-up (86.8%) occlusive results. There was no procedure-related morbidity or mortality.
CONCLUSION
By adopting different treatment strategies to different configurations and vascular sources, mirror aneurysms can be safely and effectively treated. If feasible, single-stage coil embolization should be considered as a reasonable treatment option for mirror aneurysms.
MeSH Terms
Figure
-
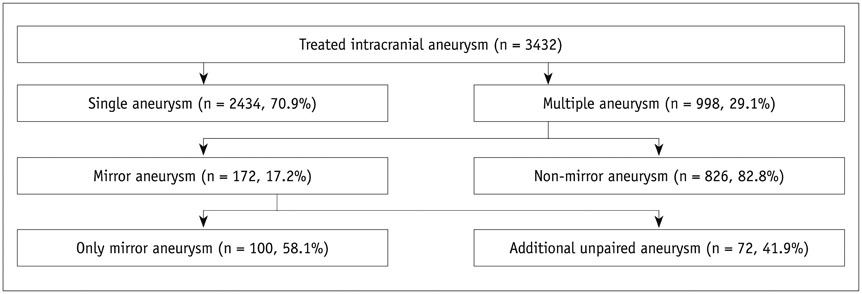
Fig. 1 Algorithm of patient population selected for study.
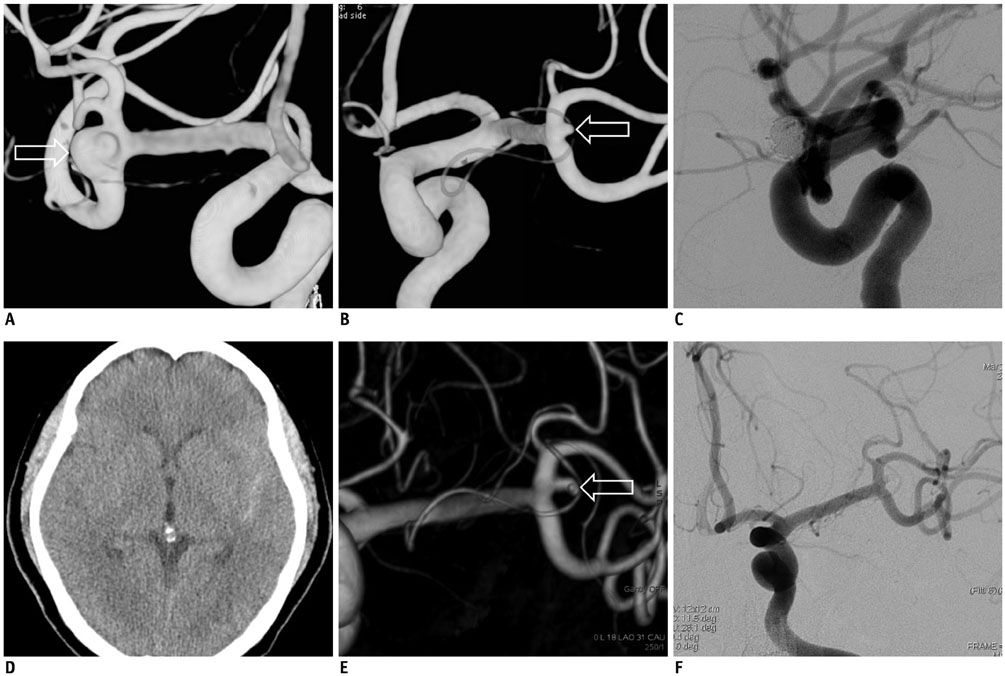
Fig. 2 Growth of untreated mirror aneurysms. Unruptured mirror aneurysms (arrows) on MCAB: three dimensional images of right (A) and left MCAB (B); coil embolization of right MCAB aneurysm (C); and observation of left MCAB aneurysms; subarachnoid hemorrhage at 11 months after coil embolization (D); significant growth (arrow) of left MCAB aneurysm (E); and completion of angiography after coil embolization (F). MCAB = middle cerebral artery bifurcation
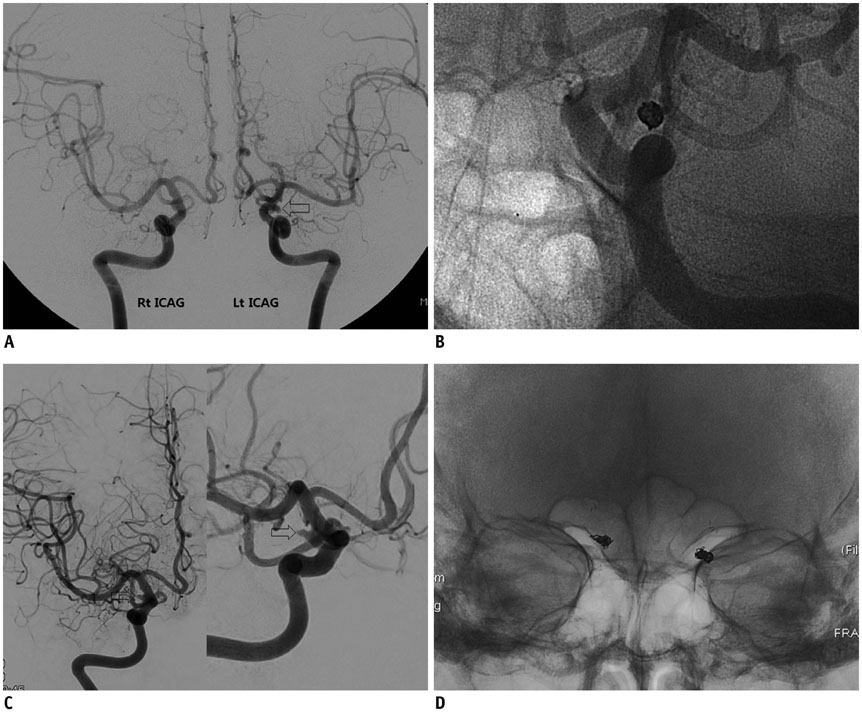
Fig. 3 De novo aneurysm at paired sites during follow-up after treatment of unilateral aneurysm. Left PcomA aneurysm (arrow) on digital subtraction angiography at baseline (A); coil embolization of left PcomA aneurysm (B); de novo right PcomA aneurysm (arrow) seen at 36 months follow-up (C); and plain radiography after coil embolization (D). ICAG = internal carotid angiography, PcomA = posterior communicating artery
Reference
-
1. Rinkel GJ. Natural history, epidemiology and screening of unruptured intracranial aneurysms. Rev Neurol (Paris). 2008; 164:781–786.
Article2. Brown RD. Unruptured intracranial aneurysms. Semin Neurol. 2010; 30:537–544.
Article3. Brown RD Jr, Broderick JP. Unruptured intracranial aneurysms: epidemiology, natural history, management options, and familial screening. Lancet Neurol. 2014; 13:393–404.
Article4. Thompson BG, Brown RD Jr, Amin-Hanjani S, Broderick JP, Cockroft KM, Connolly ES Jr, et al. Guidelines for the management of patients with unruptured intracranial aneurysms: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015; 46:2368–2400.5. Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003; 362:103–110.
Article6. Lu HT, Tan HQ, Gu BX, Wu-Wang , Li MH. Risk factors for multiple intracranial aneurysms rupture: a retrospective study. Clin Neurol Neurosurg. 2013; 115:690–694.
Article7. Ellamushi HE, Grieve JP, Jäger HR, Kitchen ND. Risk factors for the formation of multiple intracranial aneurysms. J Neurosurg. 2001; 94:728–732.
Article8. Juvela S. Risk factors for multiple intracranial aneurysms. Stroke. 2000; 31:392–397.
Article9. Kaminogo M, Yonekura M, Shibata S. Incidence and outcome of multiple intracranial aneurysms in a defined population. Stroke. 2003; 34:16–21.
Article10. Nehls DG, Flom RA, Carter LP, Spetzler RF. Multiple intracranial aneurysms: determining the site of rupture. J Neurosurg. 1985; 63:342–348.
Article11. Meissner I, Torner J, Huston J 3rd, Rajput ML, Wiebers DO, Jones LK Jr, et al. International Study of Unruptured Intracranial Aneurysms Investigators. Mirror aneurysms: a reflection on natural history. J Neurosurg. 2012; 116:1238–1241.
Article12. Lee YJ, Parreira T, Matouk CC, Menezes R, Mandell DM, terBrugge KG, et al. Clinical characteristics and preferential location of intracranial mirror aneurysms: a comparison with non-mirror multiple and single aneurysms. Neuroradiology. 2015; 57:35–40.
Article13. Wang R, Zhang D, Zhao J, Wang S, Zhao Y, Niu H. A comparative study of 43 patients with mirror-like intracranial aneurysms: risk factors, treatment, and prognosis. Neuropsychiatr Dis Treat. 2014; 10:2231–2237.14. Baccin CE, Krings T, Alvarez H, Ozanne A, Lasjaunias P. Multiple mirror-like intracranial aneurysms. Report of a case and review of the literature. Acta Neurochir (Wien). 2006; 148:1091–1095. discussion 1095.
Article15. Casimiro MV, McEvoy AW, Watkins LD, Kitchen ND. A comparison of risk factors in the etiology of mirror and nonmirror multiple intracranial aneurysms. Surg Neurol. 2004; 61:541–545.
Article16. Mehrotra A, Sharma P, Das KK, Bhaisora KS, Sardhara J, Gupta S, et al. Mirror aneurysms among multiple aneurysms: lesser of the two evils. World Neurosurg. 2016; 92:126–132.
Article17. Lesley WS. Bilateral mirror posterior inferior cerebellar artery aneurysms: diagnostic caveat on catheter angiography. J Neurointerv Surg. 2011; 3:383–385.
Article18. Xu Y, Chen SD, Lei B, Zhang WH, Wang WY. One-stage operation for rare multiple mirror intracranial aneurysms: a case report and literature review. Turk Neurosurg. 2014; 24:598–601.19. Enesi E, Rroji A, Demneri M, Vreto G, Petrela M. Mirror image distal anterior cerebral artery aneurysms treated with coil embolization. a report of two cases and literature review. Interv Neuroradiol. 2013; 19:49–55.20. Yamada K, Nakahara T, Kishida K, Yano T, Yamamoto K, Ushio Y. Multiple “mirror” aneurysms involving intracavernous carotid arteries and vertebral arteries: case report. Surg Neurol. 2000; 54:361–365.
Article21. Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003; 34:1398–1403.
Article22. Jeon JP, Cho YD, Rhim JK, Park JJ, Cho WS, Kang HS, et al. Stent-assisted coil embolization of vertebrobasilar dissecting aneurysms: procedural outcomes and factors for recanalization. Korean J Radiol. 2016; 17:801–810.
Article23. Feng Y, Wada S, Tsubota K, Yamaguchi T. The application of computer simulation in the genesis and development of intracranial aneurysms. Technol Health Care. 2005; 13:281–291.
Article24. Wang F, Xu B, Sun Z, Wu C, Zhang X. Wall shear stress in intracranial aneurysms and adjacent arteries. Neural Regen Res. 2013; 8:1007–1015.25. Munarriz PM, Gómez PA, Paredes I, Castaño-Leon AM, Cepeda S, Lagares A. Basic principles of hemodynamics and cerebral aneurysms. World Neurosurg. 2016; 88:311–319.
Article26. Hoh BL, Sistrom CL, Firment CS, Fautheree GL, Velat GJ, Whiting JH, et al. Bottleneck factor and height-width ratio: association with ruptured aneurysms in patients with multiple cerebral aneurysms. Neurosurgery. 2007; 61:716–722. discussion 722-723.27. Baumann F, Khan N, Yonekawa Y. Patient and aneurysm characteristics in multiple intracranial aneurysms. Acta Neurochir Suppl. 2008; 103:19–28.
Article28. Wang WX, Xue Z, Li L, Wu C, Zhang YY, Lou X, et al. Treatment strategies for intracranial mirror aneurysms. World Neurosurg. 2017; 100:450–458.
Article29. Rinne J, Hernesniemi J, Niskanen M, Vapalahti M. Management outcome for multiple intracranial aneurysms. Neurosurgery. 1995; 36:31–37. discussion 37-38.
Article30. Mizoi K, Suzuki J, Yoshimoto T. Surgical treatment of multiple aneurysms. Review of experience with 372 cases. Acta Neurochir (Wien). 1989; 96:8–14.31. Rodríguez-Hernández A, Gabarrós A, Lawton MT. Contralateral clipping of middle cerebral artery aneurysms: rationale, indications, and surgical technique. Neurosurgery. 2012; 71:1 Suppl Operative. 116–123. discussion 123-124.32. Wachter D, Kreitschmann-Andermahr I, Gilsbach JM, Rohde V. Early surgery of multiple versus single aneurysms after subarachnoid hemorrhage: an increased risk for cerebral vasospasm? J Neurosurg. 2011; 114:935–941.
Article33. Hong T, Wang Y. Unilateral approach to clip bilateral multiple intracranial aneurysms. Surg Neurol. 2009; 72:Suppl 1. S23–S28. discussion S28.
Article34. Santana Pereira RS, Casulari LA. Surgical treatment of bilateral multiple intracranial aneurysms. Review of a personal experience in 69 cases. J Neurosurg Sci. 2006; 50:1–8.35. Xavier AR, Rayes M, Pandey P, Tiwari A, Kansara A, Guthikonda M. The safety and efficacy of coiling multiple aneurysms in the same session. J Neurointerv Surg. 2012; 4:27–30.
Article36. Cho YD, Ahn JH, Jung SC, Kim CH, Cho WS, Kang HS, et al. Single-stage coil embolization of multiple intracranial aneurysms: technical feasibility and clinical outcomes. Clin Neuroradiol. 2016; 26:285–290.
Article37. Andic C, Aydemir F, Kardes O, Gedikoglu M, Akin S. Single-stage endovascular treatment of multiple intracranial aneurysms with combined endovascular techniques: is it safe to treat all at once? J Neurointerv Surg. 2017; 9:1069–1074.
Article38. Jing L, Liu J, Zhang Y, Paliwal N, Meng H, Wang S, et al. Analysis of multiple intracranial aneurysms with different outcomes in the same patient after endovascular treatment. World Neurosurg. 2016; 91:399–408.
Article39. Jeon P, Kim BM, Kim DJ, Kim DI, Suh SH. Treatment of multiple intracranial aneurysms with 1-stage coiling. AJNR Am J Neuroradiol. 2014; 35:1170–1173.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Analysis of Intracranial Mirror-image Aneurysms: A 20-year Single Center Experience
- Ruptured mirror DACA aneurysm: A rare case report and review of literature
- Guideline for Management of Unruptured Intracranial Aneurysms: Preliminary Report
- Endovascular treatment of intracranial aneurysms: Past and present
- Current Update on the Randomized Controlled Trials of Intracranial Aneurysms
