Endobronchial Smooth Muscle Tumors: A Series of Five Cases Highlighting Pitfalls in Diagnosis
- Affiliations
-
- 1Department of Pathology, All India Institute of Medical Sciences, New Delhi, India. deepalijain76@gmail.com
- 2Department of Pulmonary Medicine, All India Institute of Medical Sciences, New Delhi, India.
- 3Department of Otorhinolaryngology, All India Institute of Medical Sciences, New Delhi, India.
- KMID: 2417805
- DOI: http://doi.org/10.4132/jptm.2018.05.16
Abstract
- BACKGROUND
Primary endobronchial smooth muscle tumors (SMTs), which are extremely rare, include endobronchial leiomyomas and leiomyosarcomas. Clinically, SMTs present with signs and symptoms of bronchial obstruction, and lack specific radiological findings. Thus, histopathological examination is required for accurate diagnosis as well as for tumor grading. We examined the histomorphological and immunohistochemical features of endobronchial SMTs and highlighted pitfalls in diagnosis, particularly when using small biopsies.
METHODS
Cases of primary endobronchial SMTs diagnosed at our Institute over the last 6 years (2012-2017) were retrieved from the departmental archives. Histopathological features and immunohistochemistry performed for establishing the diagnosis were reviewed.
RESULTS
Five cases of SMTs occurring in endobronchial locations were identified. These included three cases of leiomyoma, and two cases of leiomyosarcoma. The age distribution of patients ranged from 13 to 65 years. Leiomyomas showed more consistent staining with smooth muscle markers (smooth muscle actin, desmin, and smooth muscle myosin heavy chain), while tumors of higher grade showed variable, focal staining, leading to erroneous diagnosis, especially on small biopsies.
CONCLUSIONS
The diagnosis of endobronchial SMTs relies on histopathological examination, for both confirmation of smooth muscle lineage and determination of the malignant potential of the lesion. Appropriate immunohistochemical panels including more than one marker of smooth muscle differentiation are extremely valuable for differential diagnosis from morphological mimics, which is necessary for instituting appropriate management.
MeSH Terms
Figure
-

Fig. 1. Clinical and radiological features in patient 1. (A) Flexible bronchoscopic image showing an endoluminal mass in the right main bronchus. (B) Coronal computed tomography reconstructed image showing a mass lesion in the right main bronchus (case 1).

Fig. 2. Leiomyoma. (A) Photomicrographs of case 3 show bronchial epithelium with a sub-epithelial spindle cell tumor arranged in fascicles. (B) Tumor cells have abundant cytoplasm and ovoid nuclei with homogeneous chromatin. (C, D) Areas of hyalinization and calcification are noted in case 2. Immunohistochemistry shows diffuse smooth muscle actin (E) and desmin positivity (F).

Fig. 3. Leiomyosarcoma. (A, B)Photomicrographs of the first biopsy from case 4 show small fragments of spindle cell tumor with mild to moderate nuclear pleomorphism and interspersed inflammatory cells; diagnosed as inflammatory myofibroblastic tumor. (C) Excision biopsy showed bronchial epithelium with a cellular spindle cell tumor in the sub-epithelial region. (D) Tumor cells have pale to bright eosinophilic cytoplasm, paranuclear vacuoles (black arrow) with interspersed inflammatory cells and pleomorphic tumor giant cells (red arrow). Immunohistochemistry shows focal positivity for smooth muscle actin (E) and desmin (F).
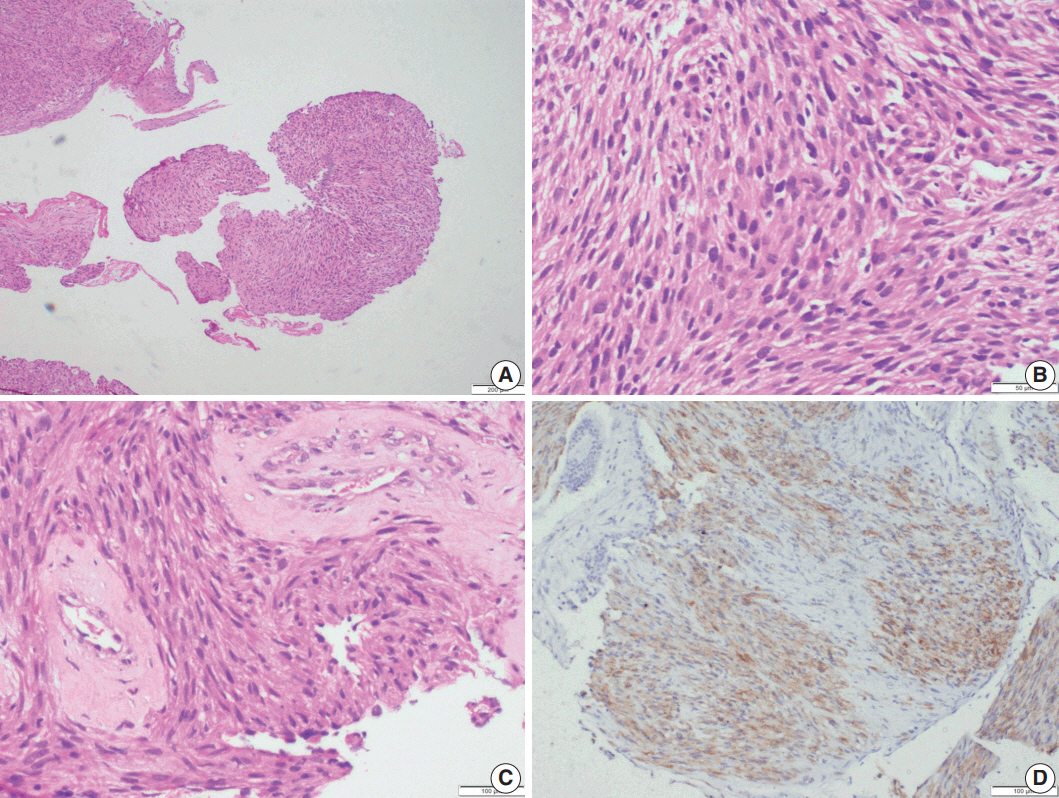
Fig. 4. Leiomyosarcoma. Photomicrographs of case 5 show multiple fragments of tumor tissue displaying a cellular spindle cell tumor (A) with moderate amounts of eosinophilic cytoplasm, ovoid, hyperchromatic nuclei, paranuclear vacuoles, and mitotic figures (B); perivascular hyalinization is noted (C). (D) Immunohistochemistry shows focal desmin positivity.
Reference
-
1. Dacic S, Elmberger G. Other mesenchymal tumours. In : Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG, editors. WHO classification of tumours of lung, pleura, thymus and heart. Lyon: IARC Press;2015. p. 132–3.2. Swarnakar R, Sinha S. Endobronchial leiomyoma: a rare and innocent tumour of the bronchial tree. Lung India. 2013; 30:57–60.
Article3. Elouazzani H, Zouaidia F, Jahid A, Bernoussi Z, Mahassini N. Primary endobronchial leiomyosarcoma of the lung: clinical, gross and microscopic findings of two cases. J Clin Imaging Sci. 2012; 2:35.
Article4. Cardenas-Garcia J, Lee-Chang A, Chung V, Shim C, Factor S, Tibb A. Bronchial leiomyoma, a case report and review of literature. Respir Med Case Rep. 2014; 12:59–62.5. Purgina B, Rao UN, Miettinen M, Pantanowitz L. AIDS-related EBV-associated smooth muscle tumors: a review of 64 published cases. Patholog Res Int. 2011; 2011:561548.6. Awasthi A, Dubey S, Sabhikhi AK, Bal S. Primary endobronchial myxoid leiomyoma in a child: an unusual case report and review of literature. Indian J Pathol Microbiol. 2016; 59:87–9.
Article7. Litzky L. Epithelial and soft tissue tumors of the tracheobronchial tree. Chest Surg Clin N Am. 2003; 13:1–40.
Article8. Lee MC, Hsu CP, Hsia JY. Surgical treatment of endobronchial leiomyosarcoma with right main bronchus total obstruction: a case report. Ann Thorac Cardiovasc Surg. 2008; 14:105–8.9. Kim YK, Kim H, Lee KS, et al. Airway leiomyoma: imaging findings and histopathologic comparisons in 13 patients. AJR Am J Roentgenol. 2007; 189:393–9.
Article10. Dmello D, Javed A, Espiritu J, Matuschak GM. Endobronchial leiomyoma: case report and literature review. J Bronchology Interv Pulmonol. 2009; 16:49–51.11. Moran CA, Suster S. Tumors of the lung and pleura. In : Fletcher CD, editor. Diagnostic histopathology of tumors. New York: Churchill Livingstone;2013. p. 207–45.12. Vaz AP, Magalhães A, Bartosch C, Fernandes G, Marques A. Primary endobronchial leiomyoma: endoscopic laser resection. Rev Port Pneumol. 2011; 17:228–31.13. Kwon YS, Kim H, Koh WJ, et al. Clinical characteristics and efficacy of bronchoscopic intervention for tracheobronchial leiomyoma. Respirology. 2008; 13:908–12.
Article14. Harris PF, Maness GM, Ward PH. Leiomyoma of the larynx and trachea: case reports. South Med J. 1967; 60:1223–7.
Article15. Lee SH, Shim JJ, Shin JS, et al. Primary endobronchial leiomyosarcoma: diagnosis following expectoration of tumor fragment. Respiration. 2001; 68:99–102.16. Attanoos RL, Appleton MA, Gibbs AR. Primary sarcomas of the lung: a clinicopathological and immunohistochemical study of 14 cases. Histopathology. 1996; 29:29–36.
Article17. Janssen JP, Mulder JJ, Wagenaar SS, Elbers HR, van den Bosch JM. Primary sarcoma of the lung: a clinical study with long-term followup. Ann Thorac Surg. 1994; 58:1151–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Smooth Muscle Tumors of the Stomach : A clinicopathologic analysis of 46 cases
- Smooth Muscle Tumors of the Stomach : A clinicopathologic analysis of 46 cases
- Smooth muscle tumors of digestive tract: a clinicopathologic study of 40 cases-
- Smooth muscle tumors of the stomach: a clinical analysis-
- A clinical study of smooth muscle tumors arising from lower GI tracts
