Intradural Procedural Time to Assess Technical Difficulty of Superciliary Keyhole and Pterional Approaches for Unruptured Middle Cerebral Artery Aneurysms
- Affiliations
-
- 1Department of Neurosurgery, Research Center for Neurosurgical Robotic Systems, Kyungpook National University, Daegu, Korea. jparkmd@hotmail.com
- KMID: 2417337
- DOI: http://doi.org/10.3340/jkns.2016.59.6.564
Abstract
OBJECTIVE
This study used the intradural procedural time to assess the overall technical difficulty involved in surgically clipping an unruptured middle cerebral artery (MCA) aneurysm via a pterional or superciliary approach. The clinical and radiological variables affecting the intradural procedural time were investigated, and the intradural procedural time compared between a superciliary keyhole approach and a pterional approach.
METHODS
During a 5.5-year period, patients with a single MCA aneurysm were enrolled in this retrospective study. The selection criteria for a superciliary keyhole approach included : 1) maximum diameter of the unruptured MCA aneurysm <15 mm, 2) neck diameter of the MCA aneurysm <10 mm, and 3) aneurysm location involving the sphenoidal or horizontal segment of MCA (M1) segment and MCA bifurcation, excluding aneurysms distal to the MCA genu. Meanwhile, the control comparison group included patients with the same selection criteria as for a superciliary approach, yet who preferred a pterional approach to avoid a postoperative facial wound or due to preoperative skin trouble in the supraorbital area. To determine the variables affecting the intradural procedural time, a multiple regression analysis was performed using such data as the patient age and gender, maximum aneurysm diameter, aneurysm neck diameter, and length of the pre-aneurysm M1 segment. In addition, the intradural procedural times were compared between the superciliary and pterional patient groups, along with the other variables.
RESULTS
A total of 160 patients underwent a superciliary (n=124) or pterional (n=36) approach for an unruptured MCA aneurysm. In the multiple regression analysis, an increase in the diameter of the aneurysm neck (p<0.001) was identified as a statistically significant factor increasing the intradural procedural time. A Pearson correlation analysis also showed a positive correlation (r=0.340) between the neck diameter and the intradural procedural time. When comparing the superciliary and pterional groups, no statistically significant between-group difference was found in terms of the intradural procedural time reflecting the technical difficulty (mean±standard deviation : 29.8±13.0 min versus 27.7±9.6 min).
CONCLUSION
A superciliary keyhole approach can be a useful alternative to a pterional approach for an unruptured MCA aneurysm with a maximum diameter <15 mm and neck diameter <10 mm, representing no more of a technical challenge. For both surgical approaches, the technical difficulty increases along with the neck diameter of the MCA aneurysm.
MeSH Terms
Figure
-
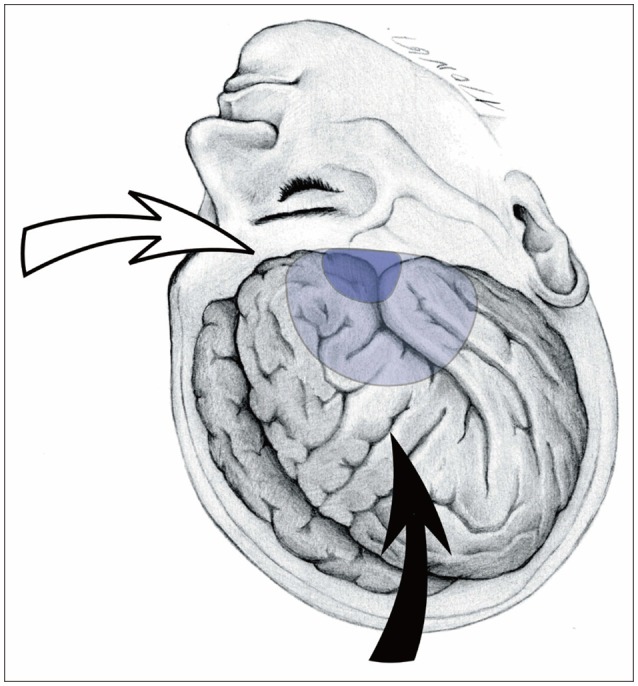
Fig. 1 Illustration showing the location of the craniotomies and microscopic direction. The surgical microscope is directed anteroinferiorly (solid arrow) with a pterional approach, while rotated and positioned in a lateral direction (empty arrow) with a superciliary approach. Note the location of the pterional craniotomy (light blue) and supraorbital mini-craniotomy (dark blue).

Fig. 2 Superciliary keyhole approach for an MCA aneurysm. A : Intraoperative photograph showing the sylvian fissure under the lesser wing (arrows) of the sphenoid via a superciliary approach. B : Intraoperative photograph showing an MCA aneurysm (arrows) exposed after focal opening in the cortical arachnoid of the sylvian fissure via a superciliary approach. MCA : middle cerebral artery.

Fig. 3 Graph of Pearson correlation analysis results, showing a positive correlation (r=0.34) between the neck diameter of the MCA aneurysm and the intradural procedural time. MCA : middle cerebral artery.
Cited by 2 articles
-
Supraorbital Keyhole Approach for Intracranial Aneurysms : Transitioning from Concerns to Confidence
Jaechan Park
J Korean Neurosurg Soc. 2020;63(1):4-13. doi: 10.3340/jkns.2019.0042.Keyhole approach in anterior circulation aneurysm: Current indication, advantages, technical limitations, complications and their avoidance
Hanuman Prajapati, Ahmad Ansari, Manish Jaiswal
J Cerebrovasc Endovasc Neurosurg. 2022;24(2):101-112. doi: 10.7461/jcen.2022.E2021.07.008.
Reference
-
1. Chalouhi N, Jabbour P, Ibrahim I, Starke RM, Younes P, El Hage G, et al. Surgical treatment of ruptured anterior circulation aneurysms : comparison of pterional and supraorbital keyhole approaches. Neurosurgery. 2013; 72:437–441. discussion 441-442. PMID: 23208062.2. Cheng CM, Noguchi A, Dogan A, Anderson GJ, Hsu FP, McMenomey SO, et al. Quantitative verification of the keyhole concept : a comparison of area of exposure in the parasellar region via supraorbital keyhole, frontotemporal pterional, and supraorbital approaches. J Neurosurg. 2013; 118:264–269. PMID: 23140145.
Article3. Czirják S, Nyáry I, Futó J, Szeifert GT. Bilateral supraorbital keyhole approach for multiple aneurysms via superciliary skin incisions. Surg Neurol. 2002; 57:314–323. discussion 323-324. PMID: 12128303.
Article4. Czirják S, Szeifert GT. Surgical experience with frontolateral keyhole craniotomy through a superciliary skin incision. Neurosurgery. 2001; 48:145–149. discussion 149-150. PMID: 11152339.
Article5. Davies JM, Lawton MT. Advances in open microsurgery for cerebral aneurysms. Neurosurgery. 2014; 74(Suppl 1):S7–S16. PMID: 24402495.
Article6. Elsharkawy A, Niemelä M, Lehečka M, Lehto H, Jahromi BR, Goehre F, et al. Focused opening of the sylvian fissure for microsurgical management of MCA aneurysms. Acta Neurochir (Wien). 2014; 156:17–25. PMID: 24101289.
Article7. Mitchell P, Vindlacheruvu RR, Mahmood K, Ashpole RD, Grivas A, Mendelow AD. Supraorbital eyebrow minicraniotomy for anterior circulation aneurysms. Surg Neurol. 2005; 63:47–51. discussion 51. PMID: 15639524.
Article8. Paladino J, Mrak G, Miklić P, Jednacak H, Mihaljević D. The keyhole concept in aneurysm surgery--a comparative study : keyhole versus standard craniotomy. Minim Invasive Neurosurg. 2005; 48:251–258. PMID: 16320184.
Article9. Park J. Superciliary keyhole approach for unruptured anterior circulation aneurysms : surgical technique, indications, and contraindications. J Korean Neurosurg Soc. 2014; 56:371–374. PMID: 25535512.
Article10. Park J, Hwang YH, Huh S, Kang DH, Kim Y. Minimally invasive and rapid surgical embolectomy (MIRSE) as rescue treatment following failed endovascular recanalization for acute ischemic stroke. Acta Neurochir (Wien). 2014; 156:2041–2049. discussion 2049. PMID: 25085542.
Article11. Park J, Hwang YH, Kim Y. Extended superciliary approach for middle cerebral artery embolectomy after unsuccessful endovascular recanalization therapy : technical note. Neurosurgery. 2009; 65:E1191–E1194. discussion E1194. PMID: 19934937.12. Park J, Kang DH, Chun BY. Superciliary keyhole surgery for unruptured posterior communicating artery aneurysms with oculomotor nerve palsy : maximizing symptomatic resolution and minimizing surgical invasiveness. J Neurosurg. 2011; 115:700–706. PMID: 21699478.
Article13. Park J, Woo H, Kang DH, Sung JK, Kim Y. Superciliary keyhole approach for small unruptured aneurysms in anterior cerebral circulation. Neurosurgery. 2011; 68(2 Suppl Operative):300–309. discussion 309. PMID: 21346651.
Article14. Reisch R, Perneczky A. Ten-year experience with the supraorbital subfrontal approach through an eyebrow skin incision. Neurosurgery. 2005; 57(4 Suppl):242–255. discussion 242-255. PMID: 16234671.
Article15. Reisch R, Stadie A, Kockro RA, Hopf N. The keyhole concept in neurosurgery. World Neurosurg. 2013; 79(2 Suppl):S17.e9–S17.e13.
Article16. Shin D, Park J. Unruptured supraclinoid internal carotid artery aneurysm surgery : superciliary keyhole approach versus pterional approach. J Korean Neurosurg Soc. 2012; 52:306–311. PMID: 23133717.
Article17. van Lindert E, Perneczky A, Fries G, Pierangeli E. The supraorbital keyhole approach to supratentorial aneurysms : concept and technique. Surg Neurol. 1998; 49:481–489. discussion 489-490. PMID: 9586924.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Superciliary Keyhole Approach for Unruptured Anterior Circulation Aneurysms: Surgical Technique, Indications, and Contraindications
- Unruptured Supraclinoid Internal Carotid Artery Aneurysm Surgery : Superciliary Keyhole Approach versus Pterional Approach
- Aneurysm Surgery Using the Superciliary Keyhole Approach
- Keyhole Approach and Neuroendoscopy for Cerebral Aneurysms
- Navigation-guided K eyhole Approach for Unruptured Intracranial Aneurysms
