Keyhole Approach and Neuroendoscopy for Cerebral Aneurysms
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Hospital, Seoul, Korea. nsdrcho@gmail.com
- 2Department of Neurosurgery, Seoul National University Boramae Medical Center, Seoul, Korea.
- 3Department of Neurosurgery, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2382760
- DOI: http://doi.org/10.3340/jkns.2017.0101.002
Abstract
- Treating diseases in the field of neurosurgery has progressed concomitantly with technical advances. Here, as a surgical armamentarium for the treatment of cerebral aneurysms, the history and present status of the keyhole approach and the use of neuroendoscopy are reviewed, including our clinical data. The major significance of keyhole approach is to expose an essential space toward a target, and to minimize brain exposure and retraction. Among several kinds of keyhole approaches, representative keyhole approaches for anterior circulation aneurysms include superciliary and lateral supraorbital, frontolateral, mini-pterional and mini-interhemispheric approaches. Because only a fixed and limited approach angle toward a target is permitted via the keyhole, however, specialized surgical devices and preoperative planning are very important. Neuroendoscopy has helped to widen the indications of keyhole approaches because it can supply illumination and visualization of structures beyond the straight line of microscopic view. In addition, endoscopic indocyanine green fluorescence angiography is useful to detect and correct any compromise of the perforators and parent arteries, and incomplete clipping. The authors think that keyhole approach and neuroendoscopy are just an intermediate step and robotic neurosurgery would be realized in the near future.
Keyword
MeSH Terms
Figure
-
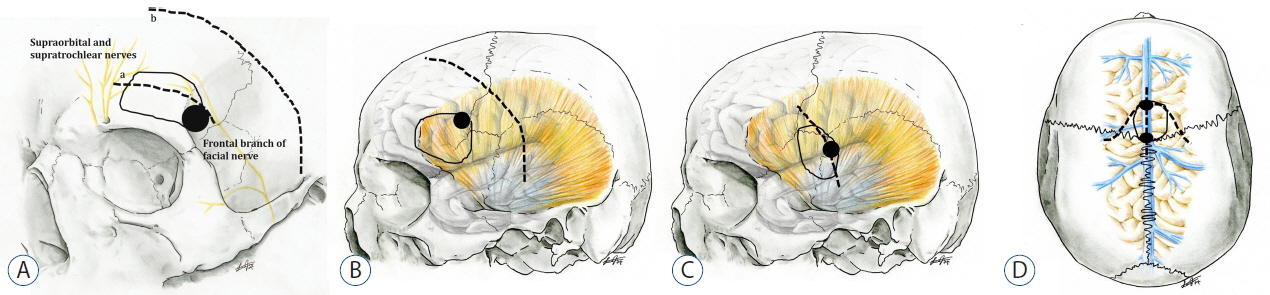
Fig. 1 Illustrations of various types of keyhole craniotomy. A: Superciliary supraorbital (a, skin incision at the upper margin of eyebrow) and frontolateral (b, skin incision just behind the hairline) keyhole craniotomy. B: Lateral supraorbital craniotomy above the sphenoid ridge, detaching the temporalis muscle. C: mini-pterional keyhole craniotomy exposing the perisylvian area. D: Mini-interhemispheric keyhole craniotomy after linear midline or inverted bowl-shaped skin incisions. Dotted lines indicate the skin incision, black circles indicate the keyhole and solid lines indicate the margin of craniotomy in a size of about 3–4 cm at each plane.
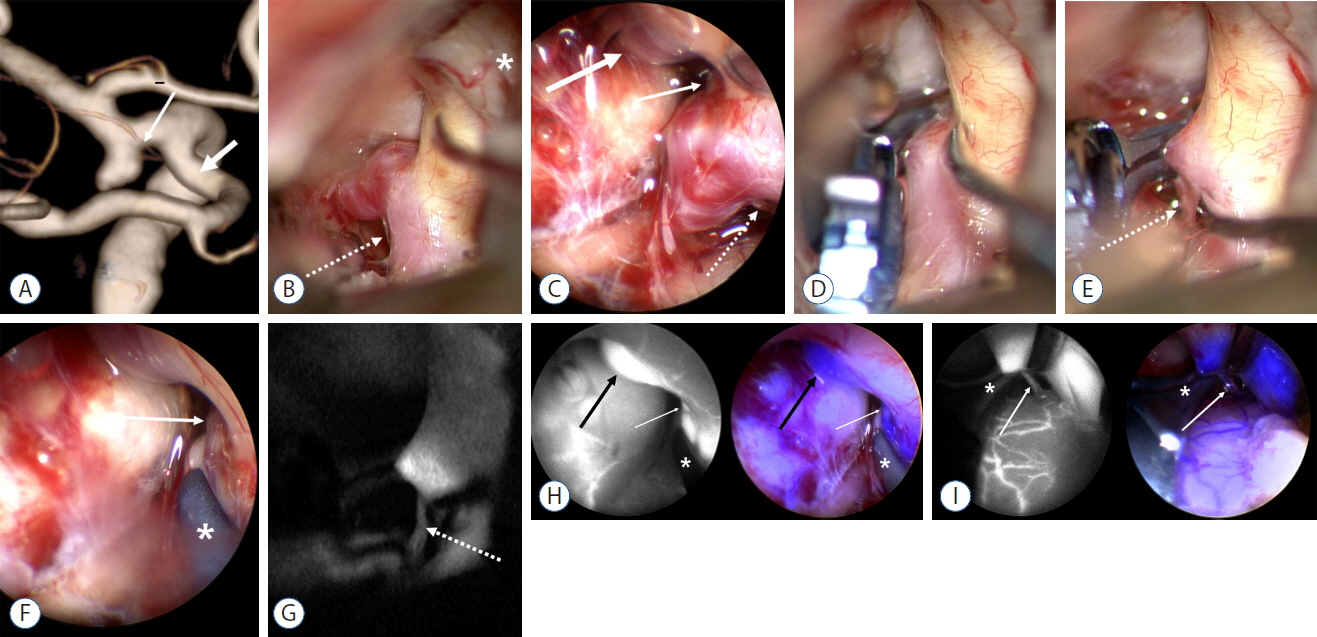
Fig. 2 A case of left anterior choroidal artery (AChA) aneurysm clipped via lateral supraorbital approach with dual channel endoscopic indocyanine green fluorescence angiography (ICGA). A: Aneurysm, AChA (thin arrow) and posterior communicating artery (PCoA, thick arrow) are seen on right lateral projection of 3D reconstructed angiography. B: AChA is not identified even retracting the internal carotid artery (asterisk: left optic nerve). However, a small perforator which seems posterior branch of AChA unseen on preoperative angiography (dotted arrow) is arising from the posterior neck of aneurysm. C: On endoscopic view, the orifices of PCoA (thick arrow), anterior (thin arrow) and posterior branches of AChA (dotted arrow) are shown. D and E: On microscopy, anterior branch of AChA is not seen even after clipping the aneurysm, however, posterior branch of AChA (dotted arrow) is demonstrated. F: On endoscopy, the orifice of anterior branch of AChA (arrow) and tip of clip blade (asterisk) are well identified. G: On microscopic ICGA in the same viewpoint of E, posterior branch of AChA (dotted arrow) is seen. H: On dual channel endoscopic ICGA of ICG image (left) and merging image (right), ICG fluorescence is visualized at the orifices of PCoA (thick black arrows) and anterior branch of AChA (thin white arrows), however not within the aneurysm (asterisk: clip blade). I: On dual channel endoscopic ICGA, ICG fluorescence is shown in posterior branch of AChA (arrow) above the clip blade (asterisk).
Cited by 1 articles
-
Effects of Scalp Nerve Block on the Quality of Recovery after Minicraniotomy for Clipping of Unruptured Intracranial Aneurysms : A Randomized Controlled Trial
Seungeun Choi, Young Hoon Choi, Hoo Seung Lee, Kyong Won Shin, Yoon Jung Kim, Hee-Pyoung Park, Won-Sang Cho, Hyongmin Oh
J Korean Neurosurg Soc. 2023;66(6):652-663. doi: 10.3340/jkns.2023.0010.
Reference
-
References
1. Apuzzo ML, Heifetz MD, Weiss MH, Kurze T. Neurosurgical endoscopy using the side-viewing telescope. J Neurosurg. 46:398–400. 1977.
Article2. Boyle WS, Smith GE. The inception of charge-coupled devices. IEEE Transact Elect Dev. 23:661–663. 1976.
Article3. Brock M, Dietz H. The small frontolateral approach for the microsurgical treatment of intracranial aneurysms. Neurochirurgia Acta (Stuttg). 21:185–191. 1978.
Article4. Bruneau M, Appelboom G, Rynkowski M, Van Cutsem N, Mine B, De Witte O. Endoscope-integrated ICG technology: first application during intracranial aneurysm surgery. Neurosurg Rev. 36:77–84. discussion 84–85. 2013.
Article5. Cha KC, Hong SC, Kim JS. Comparison between lateral supraorbital approach and pterional approach in the surgical treatment of unruptured intracranial aneurysm. J Korean Neurosurg Soc. 51:334–337. 2012.
Article6. Chalouhi N, Jabbour P, Ibrahim I, Starke RM, Younes P, El Hage G, et al. Surgical treatment of ruptured anterior circulation aneurysms: comparison of pterional and supraorbital keyhole approaches. Neurosurgery. 72:437–441. discussion 441–442. 2013.7. Cho WS, Kim JE, Kim SH, Kim HC, Kang U, Lee DS. Endoscopic fluorescence angiography with indocyanine green: a preclinical study in the swine. J Korean Neurosurg Soc. 58:513–517. 2015.
Article8. Dandy WE. Intracranial aneurysms of the internal carotid artery: cured by operation. Ann Surg. 107:654–659. 1938.
Article9. Davies JM, Lawton MT. Advances in open microsurgery for cerebral aneurysms. Neurosurgery. 74(Suppl 1):S7–S16. 2014.
Article10. Di Ieva A, Tam M, Tschabitscher M, Cusimano MD. A journey into the technical evolution of neuroendoscopy. World Neurosurg. 82:e777–e789. 2014.
Article11. Dott NM. Intracranial aneurysms cerebral arterio-radiography and surgical treatment. Edinb Med J. 40:219–234. 1933.12. Enseñat J, Alobid I, de Notaris M, Sanchez M, Valero R, Prats-Galino A, et al. Endoscopic endonasal clipping of a ruptured vertebral-posterior inferior cerebellar artery aneurysm: technical case report. Neurosurgery. 69(1 Suppl Operative):oneE121–oneE127. discussion oneE121–oneE127. 2011.13. Fischer G, Oertel J, Perneczky A. Endoscopy in aneurysm surgery. Neurosurgery. 70(2 Suppl Operative):184–190. discussion 190–191. 2012.
Article14. Fries G, Perneczky A. Endoscope-assisted brain surgery: part 2--analysis of 380 procedures. Neurosurgery. 42:226–231. discussion 231–232. 1998.
Article15. Froelich S, Cebula H, Debry C, Boyer P. Anterior communicating artery aneurysm clipped via an endoscopic endonasal approach: technical note. Neurosurgery. 68(2 Suppl Operative):310–316. discussion 315–316. 2011.
Article16. Germanwala AV, Zanation AM. Endoscopic endonasal approach for clipping of ruptured and unruptured paraclinoid cerebral aneurysms: case report. Neurosurgery. 68(1 Suppl Operative):234–239. discussion 240. 2011.
Article17. Guglielmi G, Viñuela F, Dion J, Duckwiler G. Electrothrombosis of saccular aneurysms via endovascular approach. Part 2: Preliminary clinical experience. J Neurosurg. 75:8–14. 1991.18. Hernesniemi J, Ishii K, Niemelä M, Smrcka M, Kivipelto L, Fujiki M, et al. Lateral supraorbital approach as an alternative to the classical pterional approach. Acta Neurochir Suppl. 94:17–21. 2005.
Article19. Jane JA, Park TS, Pobereskin LH, Winn HR, Butler AB. The supraorbital approach: technical note. Neurosurgery. 11:537–542. 1982.
Article20. Krayenbühl HA, Yaşargil MG, Flamm ES, Tew JM Jr. Microsurgical treatment of intracranial saccular aneurysms. J Neurosurg. 37:678–686. 1972.
Article21. Mielke D, Malinova V, Rohde V. Comparison of intraoperative microscopic and endoscopic ICG angiography in aneurysm surgery. Neurosurgery. 10(Suppl 3):418–425. discussion 425. 2014.
Article22. Mixter WJ. Ventriculoscopy and puncture of floor of third ventricle-preliminary report of a case. Boston Med Surg J. 188:277–278. 1923.23. Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, Holman R. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet. 360:1267–1274. 2002.
Article24. Nathal E, Gomez-Amador JL. Anatomic and surgical basis of the sphenoid ridge keyhole approach for cerebral aneurysms. Neurosurgery. 56(1 Suppl):178–185. discussion 178–185. 2005.
Article25. Nishiyama Y, Kinouchi H, Senbokuya N, Kato T, Kanemaru K, Yoshioka H, et al. Endoscopic indocyanine green video angiography in aneurysm surgery: an innovative method for intraoperative assessment of blood flow in vasculature hidden from microscopic view. J Neurosurg. 117:302–308. 2012.
Article26. Oppel F, Mulch G, Brock M. Endoscopic section of the sensory trigeminal root, the glossopharyngeal nerve, and the cranial part of the vagus for intractable facial pain caused by upper jaw carcinoma. Surg Neurol. 16:92–95. 1981.
Article27. Paladino J, Pirker N, Stimac D, Stern-Padovan R. Eyebrow keyhole approach in vascular neurosurgery. Minim Invasive Neurosurg. 41:200–203. 1998.
Article28. Park J, Woo H, Kang DH, Sung JK, Kim Y. Superciliary keyhole approach for small unruptured aneurysms in anterior cerebral circulation. Neurosurgery. 68(2 Suppl Operative):300–309. discussion 309. 2011.
Article29. Perneczky A, Fries G. Endoscope-assisted brain surgery: part 1-evolution, basic concept, and current technique. Neurosurgery. 42:219–224. discussion 224–225. 1998.
Article30. Perneczky A, MullerForell W, Lindert E, Fries G. Current strategies in keyhole and endoscope assisted microneurosurgery. Perneczky A, editor. Keyhole Concept in Neurosurgery. Stuttgart: Thieme Medical Publishers;1999. p. 3751.31. Prott W. Cisternoscopy of the cerebellopontine angle (author’s transl). HNO. 22:337–341. 1974.32. Raabe A, Beck J, Gerlach R, Zimmermann M, Seifert V. Near-infrared indocyanine green video angiography: a new method for intraoperative assessment of vascular flow. Neurosurgery. 52:132–139. discussion 139. 2003.
Article33. Reisch R, Fischer G, Stadie A, Kockro R, Cesnulis E, Hopf N. The supraorbital endoscopic approach for aneurysms. World Neurosurg. 82(6 Suppl):S130–S137. 2014.
Article34. Son YJ, Han DH, Kim JE. Image-guided surgery for treatment of unruptured middle cerebral artery aneurysms. Neurosurgery. 61(5 Suppl 2):266–271. discussion 271–272. 2007.
Article35. Szentirmai O, Hong Y, Mascarenhas L, Salek AA, Stieg PE, Anand VK, et al. Endoscopic endonasal clip ligation of cerebral aneurysms: an anatomical feasibility study and future directions. J Neurosurg. 124:463–468. 2016.
Article36. van Lindert E, Perneczky A, Fries G, Pierangeli E. The supraorbital keyhole approach to supratentorial aneurysms: concept and technique. Surg Neurol. 49:481–489. discussion 489–490. 1998.
Article37. Wilson DH. Limited exposure in cerebral surgery. Technical note. J Neurosurg. 34:102–106. 1971.38. Yang J, Oh CW, Kwon OK, Hwang G, Kim T, Moon JU, et al. The usefulness of the frontolateral approach as a minimally invasive corridor for clipping of anterior circulation aneurysm. J Cerebrovasc Endovasc Neurosurg. 16:235–240. 2014.
Article39. Yoshioka H, Kinouchi H. The roles of endoscope in aneurysmal surgery. Neurol Med Chir (Tokyo). 55:469–478. 2015.
Article40. Zada G, Liu C, Apuzzo ML. “Through the looking glass”: optical physics, issues, and the evolution of neuroendoscopy. World Neurosurg. 77:92–102. 2012.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Superciliary Keyhole Approach for Unruptured Anterior Circulation Aneurysms: Surgical Technique, Indications, and Contraindications
- Aneurysm Surgery Using the Superciliary Keyhole Approach
- Microsurgical Experience with Supraorbital Keyhole Operations on Anterior Circulation Aneurysms
- Navigation-guided K eyhole Approach for Unruptured Intracranial Aneurysms
- Unruptured Supraclinoid Internal Carotid Artery Aneurysm Surgery : Superciliary Keyhole Approach versus Pterional Approach
