Anatomical Variants of “Short Head of Biceps Femoris Muscle†Associated with Common Peroneal Neuropathy in Korean Populations : An MRI Based Study
- Affiliations
-
- 1Department of Neurosurgery, Chuncheon Sacred Heart Hospital, College of Medicine, Hallym University, Chuncheon, Korea. nssur771@hallym.or.kr
- 2Department of Orthopedic Surgery, Chuncheon Sacred Heart Hospital, College of Medicine, Hallym University, Chuncheon, Korea.
- 3Kangwon National University College of Medicine, Chuncheon, Korea.
- KMID: 2417328
- DOI: http://doi.org/10.3340/jkns.2018.0018
Abstract
OBJECTIVE
In Asians, kneeling and squatting are the postures that are most often induce common peroneal neuropathy. However, we could not identify a compatible compression site of the common peroneal nerve (CPN) during hyper-flexion of knees. To evaluate the course of the CPN at the popliteal area related with compressive neuropathy using magnetic resonance imaging (MRI) scans of healthy Koreans.
METHODS
1.5-Tesla knee MRI scans were obtained from enrolled patients and were retrospectively reviewed. The normal populations were divided into two groups according to the anatomical course of the CPN. Type I included subjects with the CPN situated superficial to the lateral gastocnemius muscle (LGCM). Type II included subjects with the CPN between the short head of biceps femoris muscle (SHBFM) and the LGCM. We calculated the thickness of the SHBFM and posterior elongation of this muscle, and the LGCM at the level of femoral condyles. In type II, the length of popliteal tunnel where the CPN passes was measured.
RESULTS
The 93 normal subjects were included in this study. The CPN passed through the "popliteal tunnel" formed between the SHBFM and the LGCM in 36 subjects (38.7% type II). The thicknesses of SHBFM and posterior portions of this muscle were statistically significantly increased in type II subjects. The LGCM thickness was comparable in both groups. In 78.8% of the "popliteal tunnel", a length of 21 mm to < 40 mm was measured.
CONCLUSION
In Korean population, the course of the CPN through the "popliteal tunnel" was about 40%, which is higher than the Western results. This anatomical characteristic may be helpful for understanding the mechanism of the CPNe by posture.
Keyword
MeSH Terms
Figure
-
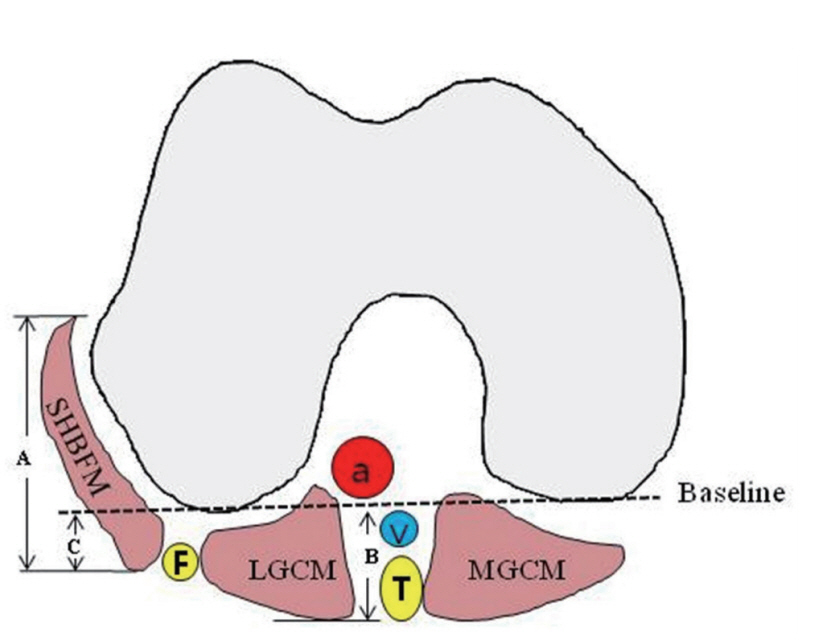
Fig. 1. Schematic description of the measurement method on the right knee. The baseline connected the two posterior apexes of the femoral condyle. The muscle thicknesses that were the vertical length of the SHBFM (A), length and maximum lengths from baseline of the LGCM (B), and the vertical and maximum length from baseline of the posterior elongated length of the SHBFM (C). a : popliteal artery, v : popliteal vein, T : tibial nerve, F : common peroneal nerve, SHBFM : short head of biceps femoris muscle, LGCM : lateral gastrocnemius muscle, MGCM : medial gastrocnemius muscle.
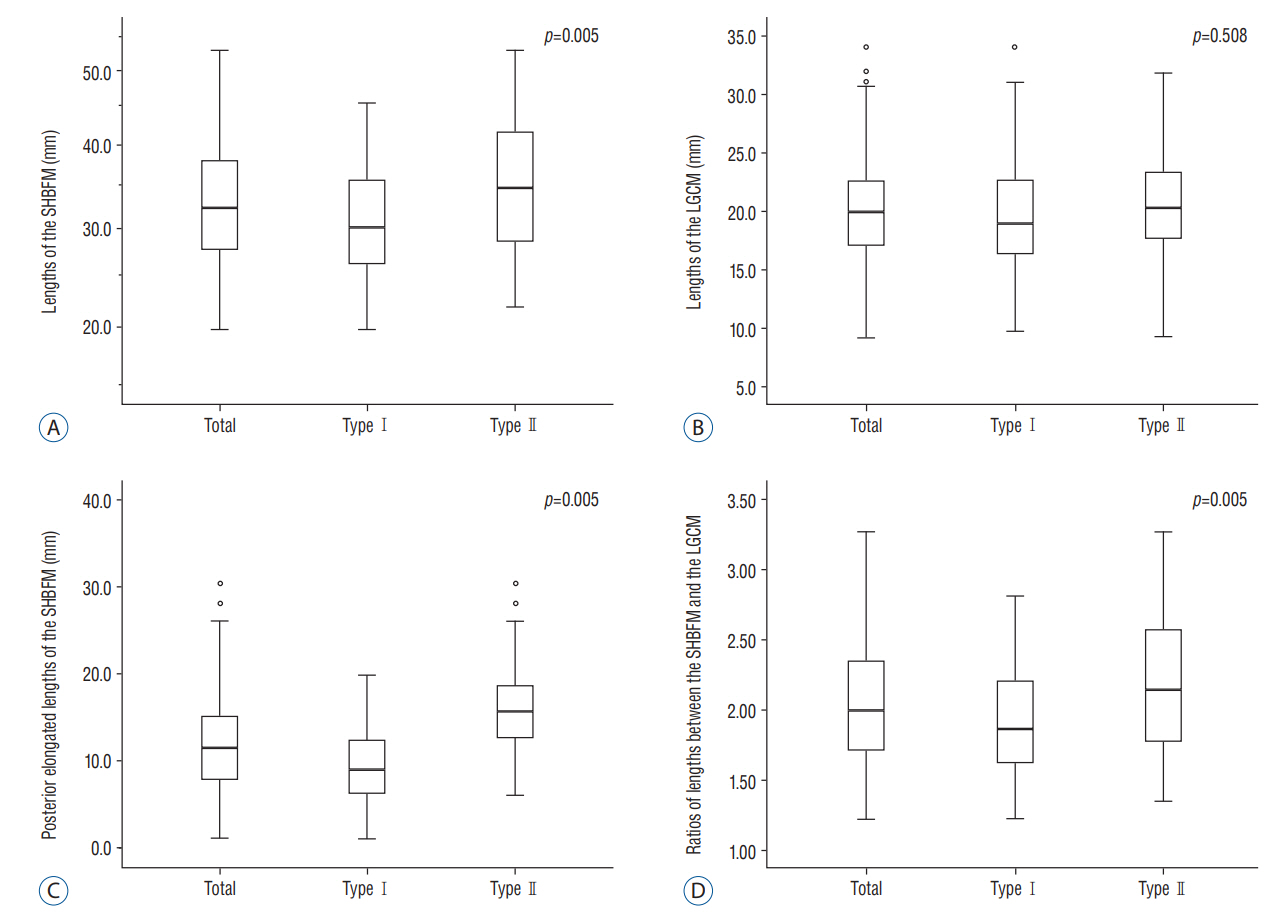
Fig. 2. Comparison of four measured thicknesses in each type. A : Comparison of measurement outcome for length of the short head of biceps femoris muscle (SHBFM) in each type. B : Comparison of measurement outcome for length of the lateral gastrocnemius muscle (LGCM) in each type. C : Comparison of measurement outcome for posterior elongated length of the SHBFM in each type. D : Ratio outcomes of lengths between the SHBFM and the LGCM in each type.
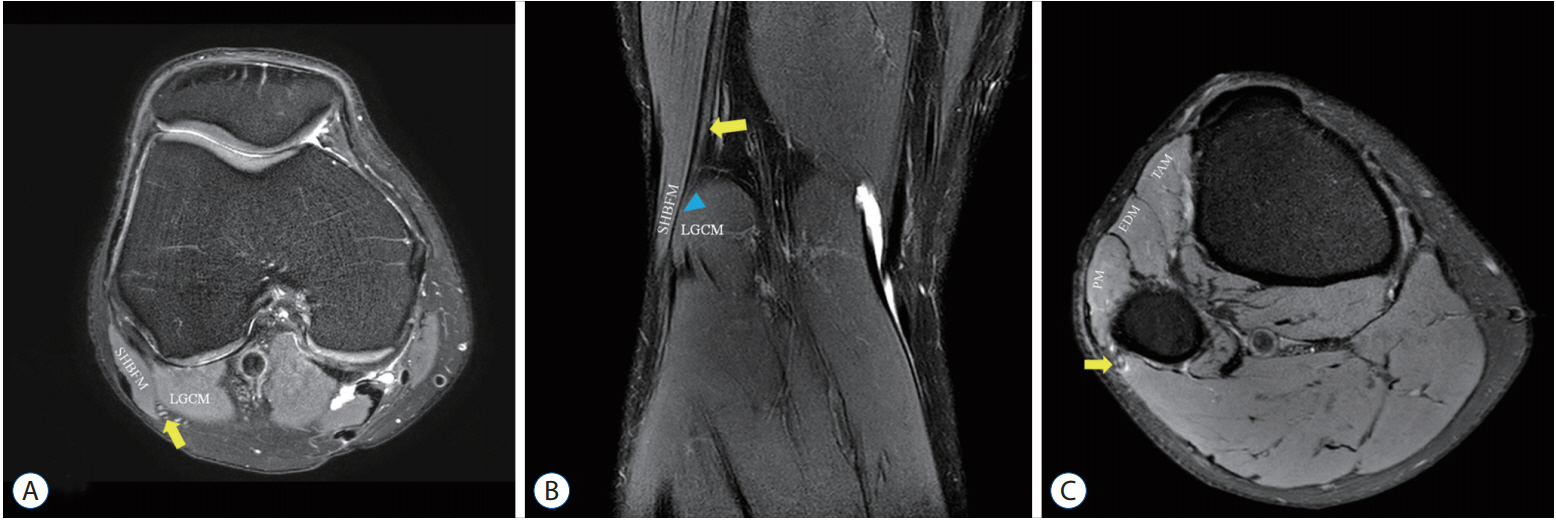
Fig. 3. Conventional 1.5T knee MRI findings. A : Axial proton density fat-saturated MRI (TR, 5100 ms; TE, 30 ms) at the level of femoral condyle was done to image the suspected course of the CPN (yellow arrow) between the SHBFM and the LGCM. B : Coronal mDIXON T2-weighted MRI (TE, 2500 ms; TE, 80 ms) revealed the CPN (yellow arrow) descending along the medial side of the SHBFM, passing through the popliteal tunnel (blue arrowhead), and traveling down to the lateral side of the fibula. The length of this tunnel was 24 mm. C : Axial fat-saturated T2-weighted MRI (TR, 3500 ms; TE, 65 ms) at the level of proximal entrance to fibular head showed the swollen CPN (yellow arrow) and demonstrated edematous high signal changes within muscles of antero-lateral compartment of lower extremity. MRI : magnetic resonance imaging, CPN : common peroneal nerve, mDIXON : modified DIXON, SHBFM : short head of biceps femoris muscle, LGCM : lateral gastrocnemius muscle, MGCM : medial gastrocnemius muscle, PM : peroneus muscle, EDM : extensor digitorum muscle group, TAM : tibialis anterior muscle.
Reference
-
References
1. Arora AK, Verma P, Abrol S. An anomalous variation in the division pattern of the common peroneal nerve. Int J Appl Basic Med Res. 1:118–119. 2011.
Article2. Deutsch A, Wyzykowski RJ, Victoroff BN. Evaluation of the anatomy of the common peroneal nerve. Defining nerve-at-risk in arthroscopically assisted lateral meniscus repair. Am J Sports Med. 27:10–15. 1999.
Article3. Donovan A, Rosenberg ZS, Cavalcanti CF. MR imaging of entrapment neuropathies of the lower extremity. Part 2. The knee, leg, ankle, and foot. Radiographics. 30:1001–1019. 2010.
Article4. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 33:159–174. 1977.
Article5. Loredo R, Hodler J, Pedowitz R, Yeh LR, Trudell D, Resnick D. MRI of the common peroneal nerve: normal anatomy and evaluation of masses associated with nerve entrapment. J Comput Assist Tomogr. 22:925–931. 1998.6. Masakado Y, Kawakami M, Suzuki K, Abe L, Ota T, Kimura A. Clinical neurophysiology in the diagnosis of peroneal nerve palsy. Keio J Med. 57:84–89. 2008.
Article7. Rempel DM, Diao E. Entrapment neuropathies: pathophysiology and pathogenesis. J Electromyogr Kinesiol. 14:71–75. 2004.
Article8. Vieira RL, Rosenberg ZS, Kiprovski K. MRI of the distal biceps femoris muscle: normal anatomy, variants, and association with common peroneal entrapment neuropathy. AJR Am J Roentgenol. 189:549–555. 2007.
Article9. Visser JJ, Hoogkamer JE, Bobbert MF, Huijing PA. Length and moment arm of human leg muscles as a function of knee and hip-joint angles. Eur J Appl Physiol Occup Physiol. 61:453–460. 1990.
Article10. Watemberg N, Amsel S, Sadeh M, Lerman-Sagie T. Common peroneal neuropathy due to surfing. J Child Neurol. 15:420–421. 2000.
Article11. Yu JK, Yang JS, Kang SH, Cho YJ. Clinical characteristics of peroneal nerve palsy by posture. J Korean Neurosurg Soc. 53:269–273. 2013.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical importance of tensor fasciae suralis arising from linea aspera along with short head of biceps femoris: a rare anomaly
- Anomalous Biceps Femoris Tendon Insertion Leading to a Snapping Knee in a Young Male
- A reproducible reference point for the common peroneal nerve during surgery at the posterolateral corner of the knee: a cadaveric study
- Common peroneal neuropathy after surgery in the lithotomy position : A case report
- The Common Peroneal Nerve Injuries
