Esophageal Artery Pseudoaneurysm and Takayasu Arteritis in a Patient with Autosomal Dominant Polycystic Kidney Disease
- Affiliations
-
- 1Department of Internal Medicine, Hallym University Medical Center, Chuncheon, Korea.
- 2Department of Internal Medicine, J Hospital, Seongnam, Korea.
- 3Department of Internal Medicine, Gangneung Dongin Hospital, Gangneung, Korea.
- 4Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
- 5Department of Internal Medicine, Seoul National University Boramae Medical Center, Seoul, Korea. yoonkyu@snu.ac.kr
- KMID: 2416374
- DOI: http://doi.org/10.5049/EBP.2018.16.1.11
Abstract
- A 47-year-old female previously diagnosed with ADPKD visited the hospital due to sudden pain in her upper abdomen and back. Esophagogastroduodenoscopy, contrast-enhanced abdominal computed tomography (CT), and CT angiography identified an esophageal artery pseudoaneurysm and hematoma in the esophagus. Urgent angiography and embolization were performed. After the procedure, CT angiography and positron emission tomography were performed due to differences in blood pressure between the arms. The patient was also found to have Takayasu arteritis and subsequently received outpatient follow-up care. The possible mechanisms that cause vascular abnormalities in ADPKD patients include damaged vascular integrity due to abnormal polycystin expression caused by PKD mutations and connective tissue abnormalities. Further research is needed to confirm these mechanisms, and ADPKD patients should be assessed for vascular abnormalities.
MeSH Terms
Figure
-
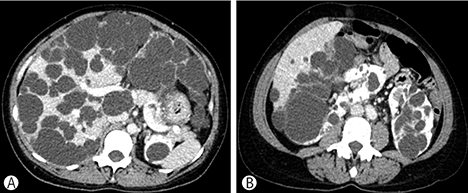
Fig. 1 Contrast-enhanced abdominopelvic computed tomography, showing numerous cysts in the liver and both kidneys.

Fig. 2 Esophagogastroduodenoscopy. External compression is noted at the lower body, antrum, and duodenal bulb (arrowheads).

Fig. 3 Computed tomography angiography, showing multifocal pseudoaneurysms (arrowheads) of the esophageal artery from the left gastric artery (arrow), with a suspected hematoma along the esophageal wall.

Fig. 4 Angiography (arteriography of the superior mesenteric artery). A 9-mm pseudoaneurysm(circle) was found in the esophageal artery and it was confirmed that it communicated with the distal left gastric artery (arrow). The distal portion of the esophageal artery was embolized and the esophageal artery was no longer seen (dashed circle) on angiography after the procedure.
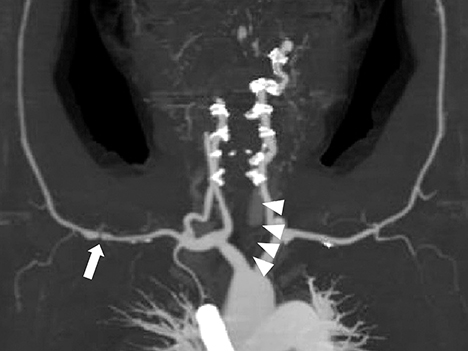
Fig. 5 Computed tomography angiography with maximum intensity projection reconstruction, showing 50%-70% luminal narrowing of the proximal right axillary artery (arrow) and near-total occlusion of the left common carotid artery from the os to the bulb (arowheads).
Reference
-
1. Gabow PA. Autosomal dominant polycystic kidney disease. N Engl J Med. 1993; 329:332–342.
Article2. Perrone RD, Malek AM, Watnick T. Vascular complications in autosomal dominant polycystic kidney disease. Nat Rev Nephrol. 2015; 11:589–598.
Article3. Ecder T, Schrier RW. Cardiovascular abnormalities in autosomal-dominant polycystic kidney disease. Nat Rev Nephrol. 2009; 5:221–228.
Article4. Uğur M, Ersoy E, Oztepe B, Kinay E, Sezer S. Rare Etiology of Gastrointestinal Bleeding: Polycystic Kidney Disease. Gavin J Urol Renal Dis. 2016; 2016:13–15.5. de Souza AWS, de Carvalho JF. Diagnostic and classification criteria of Takayasu arteritis. J Autoimmun. 2014; 48:79–83.
Article6. Matsumura K, Hirano T, Takeda K, Matsuda A, Nakagawa T, Yamaguchi N, et al. Incidence of aneurysms in Takayasu's arteritis. Angiology. 1991; 42:308–315.
Article7. Matsumoto T, Ishizuka M, Iso Y, Kita J, Kubota K. Mini-Laparotomy for Superior Mesenteric Artery Aneurysm Due to Takayasu's Arteritis. Int Surg. 2015; 100:765–769.
Article8. Sung PH, Yang YH, Chiang HJ, Chiang JY, Chen CJ, Liu CT, et al. Risk of aortic aneurysm and dissection in patients with autosomal-dominant polycystic kidney disease: a nationwide population-based cohort study. Oncotarget. 2017; 8:57594.
Article9. Igarashi P, Somlo S. Genetics and pathogenesis of polycystic kidney disease. J Am Soc Nephrol. 2002; 13:2384–2398.
Article10. Graf S, Schischma A, Eberhardt KE, Istel R, Stiasny B, Schulze BD. Intracranial aneurysms and dolichoectasia in autosomal dominant polycystic kidney disease. Nephrol Dial Transplant. 2002; 17:819–823.
Article11. Ul Haque A. Adult polycystic kidney disease: a disorder of connective tissue? Int J Clin Exp Pathol. 2008; 1:84.12. Nakagawa S, Furuichi K, Sagara A, Shinozaki Y, Kitajima S, Toyama T, et al. An autopsy case of vertebrobasilar dolichoectasia under hemodialysis due to autosomal dominant polycystic kidney disease. CEN Case Rep. 2016; 5:51–55.
Article13. Serra R, Butrico L, Fugetto F, Chibireva MD, Malva A, De Caridi G, et al. Updates in Pathophysiology, Diagnosis and Management of Takayasu Arteritis. Ann Vasc Surg. 2016; 35:210–225.
Article14. Arend WP, Michel BA, Bloch DA, Hunder GG, Calabrese LH, Edworthy SM, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 33:1129–1134.
Article15. van Rijn MJ, ten Raa S, Hendriks J, Verhagen H. Visceral aneurysms: Old paradigms, new insights? Best Pract Res Clin Gastroenterol. 2017; 31:97–104.
Article16. Baek HJ, Shin KC, Lee YJ, Kang SW, Lee EB, Song YW. Takayasu's arteritis concurrent with Marfan syndrome--a case report. Angiology. 2000; 51:435–439.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Takayasu's Arteritis Associated with Subarachnoid Hemorrhage and Intracranial Aneurysm: Case Report
- A Case of Renal Cell Carcinoma in Autosomal Dominant Polycystic Kidney Disease Hemodialyzed
- A Case of Non ST Elevation Myocardial Infarction by Coronary Artery Focal Spasm in a Patient with Autosomal Dominant Polycystic Kidney Disease
- Segmental Cystic Disease of the Kidney: A Case Report
- Autosomal Dominant Polycystic Kidney Disease: 2009 Update for Internists
