MRI Findings of an Ampulla of Vater Neuroendocrine Tumor with Liver and Lymph Node Metastasis: a Case Report
- Affiliations
-
- 1Department of Radiology, Dankook University Hospital, Dankook University School of Medicine, Cheonan, Korea. deepva@hanmail.net
- 2Department of Pathology, Dankook University Hospital, Dankook University School of Medicine, Cheonan, Korea.
- KMID: 2415892
- DOI: http://doi.org/10.13104/imri.2018.22.2.123
Abstract
- An ampulla of Vater neuroendocrine tumor (AOV-NET) is a rare subset of gastroenteropancreatic neuroendocrine tumors (GEP-NETs). Very few studies have been undertaken regarding MRI findings of an AOV-NET. We report on a case of a 59-year-old woman diagnosed with an AOV-NET with liver and lymph node metastasis, with an emphasis on the MRI findings. This case shows rare and precious typical MRI findings of an AOV-NET. The MRI visualized the AOV-NET very well and is helpful for the differentiation of an AOV-NET from other tumors in the ampullary area as well as with treatment planning.
MeSH Terms
Figure
-

Fig. 1. A 59-year-old woman with an ampulla of Vater (AOV) neuroendocrine tumor. The enhanced pancreatic phase abdominal CT images show (a) a 1.5 cm mass (arrow) with avid, homogeneous enhancement at the AOV, (b) a 9.7 cm lobulated enhancing mass with multifocal low attenuating cystic or necrotic change in the right hepatic lobe and (c) a 2.3 cm enlarged lymph node (arrow) with central necrotic change was noted in the left paraaortic area.
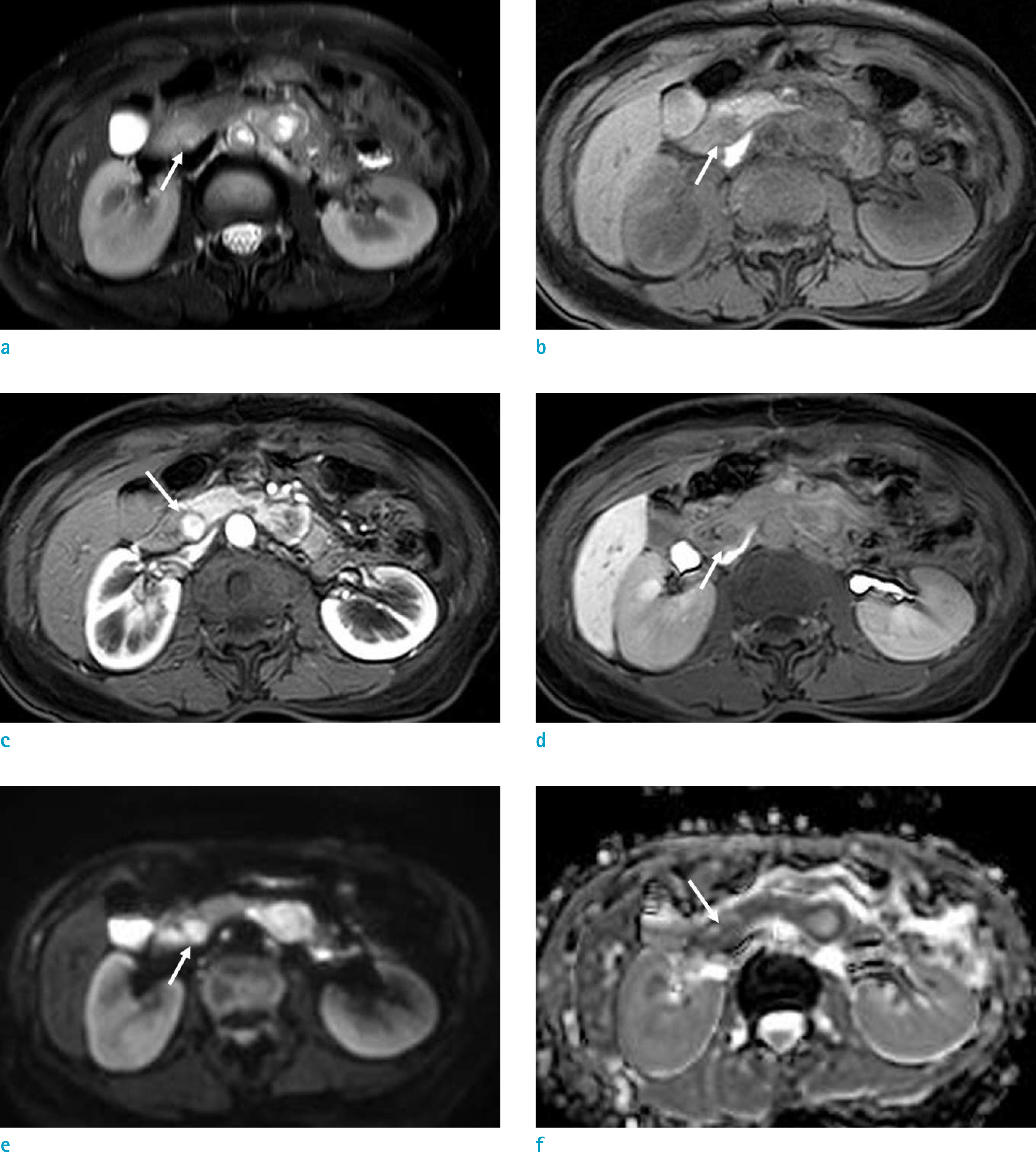
Fig. 2. An ampulla of Vater (AOV) neuroendocrine tumor in a 59-year-old woman. A 1.5 cm sized round mass in the AOV (arrow) showed slightly high signal intensity when compared with a pancreatic parenchyma on a T2-weighted image (a) and low signal intensity on a T1-weighted image (b). On the enhanced MRI, using GD-EOB-DTPA (Primovist), the AOV mass (arrow) showed avid, homogeneous enhancement on the arterial phase (c) with isosignal intensity when compared with a pancreatic parenchyma on the delayed phase (d). The AOV mass (arrow) exhibited high signal intensity on a high b value diffusion weighted image (e) without a definitive low apparent diffusion coefficient value (f).

Fig. 3. A metastatic hepatic mass in a 59-year-old woman. The single hepatic mass showed a ring like, radial appearance, strong enhancement with multifocal low signal intensity cystic portions on the arterial phase (a) of enhanced MRI. The hepatic mass showed heterogeneous isosignal intensity, than liver parenchyma on the portal-venous phase (b), washout on the delayed phase (c) and low signal intensity on the hepatobiliary phase (d). There were multifocal bright signal intensity cystic lesions in the hepatic mass on a T2-weighted image (e). The hepatic mass showed high signal intensity on a diffusion weighted image (f) without a definite low apparent diffusion coefficient value (g).
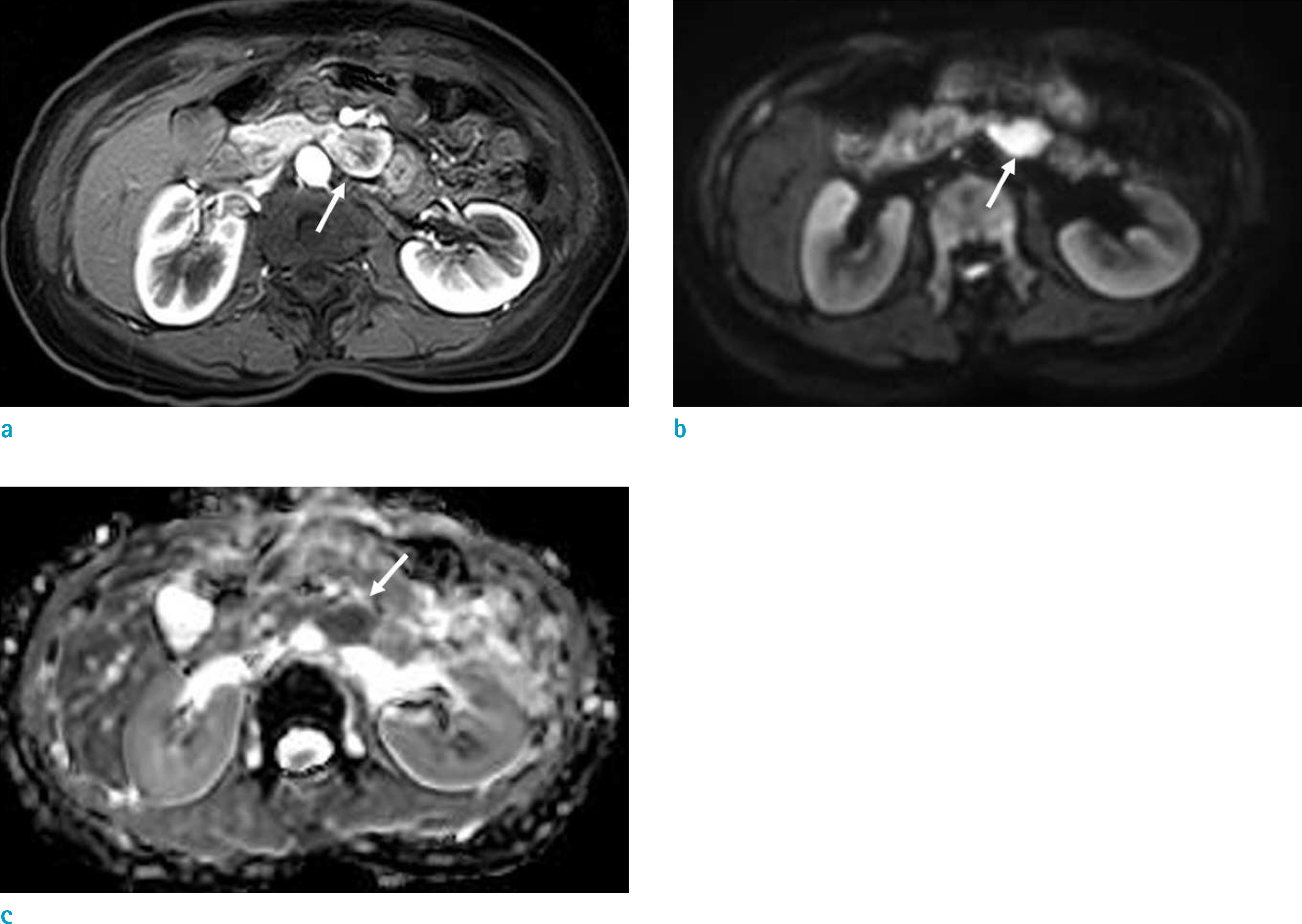
Fig. 4. A metastatic paraaortic lymph node in a 59-year-old woman. An enlarged lymph node (arrow) with a central necrotic portion was noted in the left paraaortic area. This lymph node showed prominent enhancement on the arterial phase of an enhanced MRI (a). The enhanced portion of this lymph node (arrow) showed high signal intensity on a diffusion weighted image (b) and a low apparent diffusion coefficient value (c).

Fig. 5. The gross specimen and microscopic examination. The gross specimen showed (a) a 1.5 cm well-demarcated whitish solid mass at the ampulla of Vater (AOV) and (b) a 9.0 cm well-demarcated red tan mass with a fish-flesh consistency in the right hepatic lobe. Upon microscopic examination (Hematoxylin & Eosin staining, × 100), the tumor cells of the AOV mass showed (c) a nested, trabecular growth pattern and had moderate amounts of cytoplasm and round nuclei. Immunostaining for synaptophysin was positive in the tumor cells (d).
Reference
-
References
1. Sahani DV, Bonaffini PA, Fernandez-Del Castillo C, Blake MA. Gastroenteropancreatic neuroendocrine tumors: role of imaging in diagnosis and management. Radiology. 2013; 266:38–61.
Article2. Jayant M, Punia R, Kaushik R, et al. Neuroendocrine tumors of the ampulla of vater: presentation, pathology and prognosis. JOP. 2012; 13:263–267.3. Carter JT, Grenert JP, Rubenstein L, Stewart L, Way LW. Neuroendocrine tumors of the ampulla of Vater: biological behavior and surgical management. Arch Surg. 2009; 144:527–531.4. Dumitrascu T, Dima S, Herlea V, Tomulescu V, Ionescu M, Popescu I. Neuroendocrine tumours of the ampulla of Vater: clinicopathological features, surgical approach and assessment of prognosis. Langenbecks Arch Surg. 2012; 397:933–943.
Article5. Yang K, Yun SP, Kim S, Shin N, Park DY, Seo HI. Clinicopathological features and surgical outcomes of neuroendocrine tumors of ampulla of Vater. BMC Gastroenterol. 2017; 17:70.
Article6. Raman SP, Fishman EK. Abnormalities of the distal common bile duct and ampulla: diagnostic approach and differential diagnosis using multiplanar reformations and 3D imaging. AJR Am J Roentgenol. 2014; 203:17–28.
Article7. Lewis RB, Lattin GE Jr, Paal E. Pancreatic endocrine tumors: radiologic-clinicopathologic correlation. Radiographics. 2010; 30:1445–1464.
Article8. Tsukagoshi M, Hosouchi Y, Araki K, et al. Neuroendocrine tumor of the ampulla of Vater with distant cystic lymph node metastasis: a case report. Surg Case Rep. 2016; 2:73.
Article9. Saeed A, Buell JF, Kandil E. Surgical treatment of liver metastases in patients with neuroendocrine tumors. Ann Transl Med. 2013; 1:6.10. Dromain C, de Baere T, Baudin E, et al. MR imaging of hepatic metastases caused by neuroendocrine tumors: comparing four techniques. AJR Am J Roentgenol. 2003; 180:121–128.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of a Collision Tumor in the Ampulla of Vater with an Adenocarcinoma and a Large Cell Neuroendocrine Carcinoma
- Prognostic value of the lymph node metastasis in patients with ampulla of Vater cancer after surgical resection
- Collision tumor of the ampulla of Vater - Coexistence of neuroendocrine carcinoma and adenocarcinoma: report of a case
- Computed Tomographic Findings of the Carcinoma of the Ampulla of Vater
- Carcinoid of the Ampulla of Vater: A Case Report
