Correction of Eyes and Lip Canting after Bimaxillary Orthognathic Surgery
- Affiliations
-
- 1Institute for Human Tissue Restoration, Department of Plastic & Reconstructive Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. dhlew@yuhs.ac
- 2Lee Jina Dental Clinic, Seoul, Korea.
- KMID: 2415539
- DOI: http://doi.org/10.3349/ymj.2018.59.6.793
Abstract
- Patients who have a lower facial asymmetry with compensatory head posture (developmental facial asymmetry) may have minor temporomandibular (T-M) joint problems and tend to mask their asymmetry by tilting the head for camouflage of their chin deviation. However, this compensatory head posture can give the impression of orbital dystopia and c spine deviation. When these patients undergo bimaxillary orthognathic surgery, orbital canting and head tilting improves gradually without the need for camouflage, and bleary eyes become clearer. We evaluated 13 patients who underwent LeFort I osteotomy combined with bilateral sagittal split osteotomy of the mandible for developmental facial asymmetry to quantitatively observe whole facial postural changes after surgery. Pre-operative and post-operative 1:1 full-face photographs of the patients were analyzed to compare the degrees of head tilting and orbital canting and the sizes of the eye opening. After bimaxillary orthognathic surgery, eye canting decreased from 2.6° to 1.5°, eye and lip lines came closer to parallel, and the degree of head tilting decreased from 3.4° to 1.3°. The eyes also appeared to open wider. Correction of lower facial skeletal asymmetry through bimaxillary orthognathic surgery improved head tilting and orbital canting gradually by eliminating the need of compensatory head posture. Facial expressions also changed as the size of the eyes increased due to the reduction of facial muscle tension caused by T-M joint dysfunction.
MeSH Terms
Figure
-
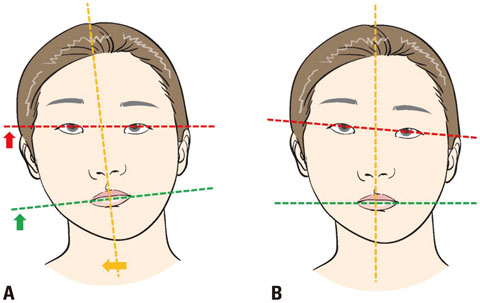
Fig. 1 Schematic illustrations. (A) Natural head position. In the natural head position with a horizontal visual axis, a difference in height of the oral commissures is apparent. (B) Compensatory head posture. Tilting the head camouflages the lower face asymmetry, but results in canting of the orbital plane.
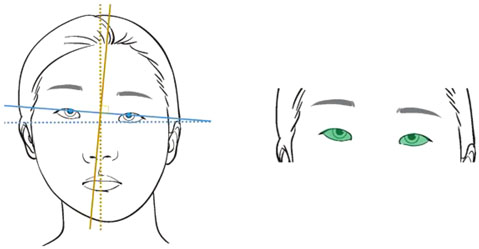
Fig. 2 In the compensatory head position, orbital canting was evaluated as the angle between true horizontal (left, dotted blue line) and the line connecting the centers of the pupils (left, linear blue line). The opening of the eye was calculated using the ImageJ program (National Institute of Health) by tracing the margin along the upper and lower eyelid (right, green area). Head tilting was evaluated as the angle between true vertical (left, dotted yellow line) and the line perpendicular to the interpupillary line (left, linear yellow line).

Fig. 3 The degree of orbital canting decreased by 42.8% (A). Eye opening area became wider after surgery but was not statistically significant (B). The degree of head tilting decreased by 60.6% (C). *p<0.05.
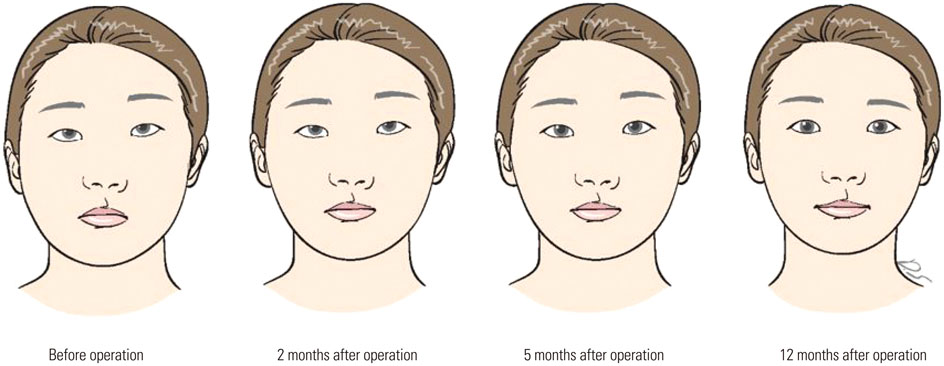
Fig. 4 Schematic illustrations reflect changes in appearance gradually over the 12-month postoperative period.
Reference
-
1. Kim YH, Jeon J, Rhee JT, Hong J. Change of lip cant after bimaxillary orthognathic surgery. J Oral Maxillofac Surg. 2010; 68:1106–1111.
Article2. Padwa BL, Kaiser MO, Kaban LB. Occlusal cant in the frontal plane as a reflection of facial asymmetry. J Oral Maxillofac Surg. 1997; 55:811–816.
Article3. Capurso U, Garino GB, Rotolo L, Verna C. [Radiographic screening of asymmetry and postural changes in orthodontic patients]. Mondo Ortod. 1990; 15:313–320.4. van Keulen C, Martens G, Dermaut L. Unilateral posterior crossbite and chin deviation: is there a correlation? Eur J Orthod. 2004; 26:283–288.
Article5. Song WC, Koh KS, Kim SH, Hu KS, Kim HJ, Park JC, et al. Horizontal angular asymmetry of the face in korean young adults with reference to the eye and mouth. J Oral Maxillofac Surg. 2007; 65:2164–2168.
Article6. Lee DH, Yu HS. Masseter muscle changes following orthognathic surgery: a long-term three-dimensional computed tomography follow-up. Angle Orthod. 2012; 82:792–798.7. Isacsson G, Linde C, Isberg A. Subjective symptoms in patients with temporomandibular joint disk displacement versus patients with myogenic craniomandibular disorders. J Prosthet Dent. 1989; 61:70–77.
Article8. D'Attilio M, Epifania E, Ciuffolo F, Salini V, Filippi MR, Dolci M, et al. Cervical lordosis angle measured on lateral cephalograms; findings in skeletal class II female subjects with and without TMD: a cross sectional study. Cranio. 2004; 22:27–44.9. Gremillion HA. The prevalence and etiology of temporomandibular disorders and orofacial pain. Tex Dent J. 2000; 117:30–39.10. Lee WY, Okeson JP, Lindroth J. The relationship between forward head posture and temporomandibular disorders. J Orofac Pain. 1995; 9:161–167.11. Munhoz WC, Marques AP, Siqueira JT. Radiographic evaluation of cervical spine of subjects with temporomandibular joint internal disorder. Braz Oral Res. 2004; 18:283–289.
Article12. Bjork A. Some biological aspects of prognathism and occlusion of the teeth. Acta Odontol Scand. 1950; 9:1–40.
Article13. Marcotte MR. Head posture and dentofacial proportions. Angle Orthod. 1981; 51:208–213.14. Di Palma E, Gasparini G, Pelo S, Tartaglia GM, Sforza C. Activities of masticatory muscles in patients before orthognathic surgery. J Craniofac Surg. 2010; 21:724–726.
Article15. Goto TK, Nishida S, Yahagi M, Langenbach GE, Nakamura Y, Tokumori K, et al. Size and orientation of masticatory muscles in patients with mandibular laterognathism. J Dent Res. 2006; 85:552–556.
Article16. Kiliaridis S, Katsaros C. The effects of myotonic dystrophy and Duchenne muscular dystrophy on the orofacial muscles and dentofacial morphology. Acta Odontol Scand. 1998; 56:369–374.
Article17. Sims AB, Stack BC, Demerjian GG. Spasmodic torticollis: the dental connection. Cranio. 2012; 30:188–193.
Article18. Monaco A, Streni O, Marci MC, Sabetti L, Marzo G, Giannoni M. Relationship between mandibular deviation and ocular convergence. J Clin Pediatr Dent. 2004; 28:135–138.
Article19. Shapiro IJ. Relation between vertical facial asymmetry and postural changes of the spine and ancillary muscles. Optom Vis Sci. 1994; 71:529–538.
Article20. Marinetti CJ. The lower muscular balance of the face used to lift labial commissures. Plast Reconstr Surg. 1999; 104:1153–1162.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Change of lip canting after bimaxillary orthognathic surgery
- Correction of Lip Canting Using Bioabsorbables during Orthognathic Surgery
- Horizontal change of philtrum after orthognathic surgery in patients with facial asymmetry
- Three-dimensional evaluation of the correlation between lip canting and craniofacial planes
- The effect of orthognathic surgery on the lip lines while smiling in skeletal class III patients with facial asymmetry
