Investig Clin Urol.
2018 Jul;59(4):275-279. 10.4111/icu.2018.59.4.275.
Proof of concept: Exposing the myth of urethral atrophy after artificial urinary sphincter via assessment of circumferential recovery after capsulotomy and intraoperative pressure profiling of the pressure regulating balloon
- Affiliations
-
- 1Department of Urology, Wake Forest Baptist Medical Center, Winston-Salem, NC, USA. amympearlman@gmail.com
- 2Department of Urology, University of Kentucky, Lexington, KY, USA.
- KMID: 2414761
- DOI: http://doi.org/10.4111/icu.2018.59.4.275
Abstract
- PURPOSE
Rate of continence after artificial urinary sphincter (AUS) placement appears to decline with time. After appropriate workup to exclude inadvertent device deactivation, development of urge or overflow incontinence, and fluid loss, many assume recurrent stress urinary incontinence (rSUI) to be secondary to nonmechanical failure, asserting urethral atrophy as the etiology. We aimed to characterize the extent of circumferential urethral recovery following capsulotomy and that of pressure regulating balloon (PRB) material fatigue in men undergoing AUS revision for rSUI.
MATERIALS AND METHODS
Retrospective review of a single surgeon database was performed. Cases of AUS removal/replacement for rSUI involving ventral subcuff capsulotomy and intraoperative PRB pressure profile assessments were identified.
RESULTS
The described operative approach involving capsulotomy was applied in 7 patients from November 2015 to September 2017. Mean patient age was 75 years. Mean time between AUS placement and revision was 103 months. Urethral circumference increased in all patients after capsulotomy (mean increase 1.1 cm; range 0.5-2.5 cm). Cuff size increased, remained the same, and decreased in 2, 3, and 2 patients, respectively. Six of 7 patients underwent PRB interrogation. Four of these 6 PRBs (66.7%) demonstrated pressures in a category below the reported range of the original manufacturer rating.
CONCLUSIONS
Despite visual appearance to suggest urethral atrophy, subcuff capsulotomy results in increased urethral circumference in all patients. Furthermore, intraoperative PRB profiling demonstrates material fatigue. Future multicenter efforts are warranted to determine if capsulotomy, with or without PRB replacement, may simplify surgical management of rSUI with reductions in cost and/or morbidity.
MeSH Terms
Figure
-
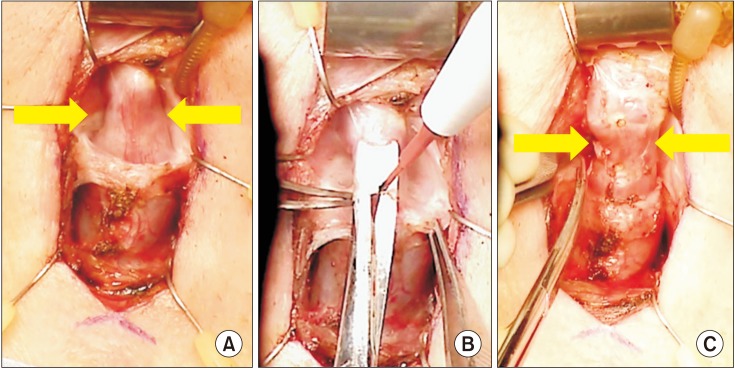
Fig. 1 (A) Urethra at site of initial cuff placement prior to capsulotomy with 3 cm urethral circumference. (B) Ventral capsulotomy performed via combination of sharp dissection and electrocautery. (C) Urethra at site of initial cuff placement after capsulotomy measuring 4 cm in urethral circumference, demonstrating restoration of urethral circumference.
Reference
-
1. Montague DK. Evolution of implanted devices for urinary incontinence. Cleve Clin Q. 1984; 51:405–409. PMID: 6467600.
Article2. Raj GV, Peterson AC, Toh KL, Webster GD. Outcomes following revisions and secondary implantation of the artificial urinary sphincter. J Urol. 2005; 173:1242–1245. PMID: 15758761.
Article3. Litwiller SE, Kim KB, Fone PD, White RW, Stone AR. Postprostatectomy incontinence and the artificial urinary sphincter: a long-term study of patient satisfaction and criteria for success. J Urol. 1996; 156:1975–1980. PMID: 8911369.
Article4. Viers BR, Linder BJ, Rivera ME, Rangel LJ, Ziegelmann MJ, Elliott DS. Long-term quality of life and functional outcomes among primary and secondary artificial urinary sphincter implantations in men with stress urinary incontinence. J Urol. 2016; 196:838–843. PMID: 26997310.5. Van der Aa F, Drake MJ, Kasyan GR, Petrolekas A, Cornu JN. Young Academic Urologists Functional Urology Group. The artificial urinary sphincter after a quarter of a century: a critical systematic review of its use in male non-neurogenic incontinence. Eur Urol. 2013; 63:681–689. PMID: 23219375.
Article6. Montague DK, Angermeier KW. Artificial urinary sphincter troubleshooting. Urology. 2001; 58:779–782. PMID: 11711363.
Article7. Eswara JR, Chan R, Vetter JM, Lai HH, Boone TB, Brandes SB. Revision techniques after artificial urinary sphincter failure in men: results from a multicenter study. Urology. 2015; 86:176–180. PMID: 26142602.
Article8. DiMarco DS, Elliott DS. Tandem cuff artificial urinary sphincter as a salvage procedure following failed primary sphincter placement for the treatment of post-prostatectomy incontinence. J Urol. 2003; 170:1252–1254. PMID: 14501735.
Article9. O'Connor RC, Lyon MB, Guralnick ML, Bales GT. Long-term follow-up of single versus double cuff artificial urinary sphincter insertion for the treatment of severe postprostatectomy stress urinary incontinence. Urology. 2008; 71:90–93. PMID: 18242372.10. Collado Serra A, Domínguez-Escrig J, Gómez-Ferrer Á, Batista Miranda E, Rubio-Briones J, Solsona Narbón E. Prospective follow-up study of artificial urinary sphincter placement preserving the bulbospongiosus muscle. Neurourol Urodyn. 2017; 36:1387–1394. PMID: 27654121.
Article11. Rahman NU, Minor TX, Deng D, Lue TF. Combined external urethral bulking and artificial urinary sphincter for urethral atrophy and stress urinary incontinence. BJU Int. 2005; 95:824–826. PMID: 15794791.
Article12. Wiedemann L, Cornu JN, Haab E, Peyrat L, Beley S, Cathelineau X, et al. Transcorporal artificial urinary sphincter implantation as a salvage surgical procedure for challenging cases of male stress urinary incontinence: surgical technique and functional outcomes in a contemporary series. BJU Int. 2013; 112:1163–1168. PMID: 24053170.
Article13. Guralnick ML, Miller E, Toh KL, Webster GD. Transcorporal artificial urinary sphincter cuff placement in cases requiring revision for erosion and urethral atrophy. J Urol. 2002; 167:2075–2078. discussion 2079. PMID: 11956443.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Urinary Incontinence Treatment Using AMS 800-Artificial Sphincter
- Dynamic Urethral Pressure Profilometry using Triple Lumen Urodynamic Catheter
- A Case of Urinary Incontinence Treated with AMS 800 Artificial Sphincter
- Effect of Transrectal Probe Insertion on the Opening of Internal Urethral Sphincter
- A Study of Urodynamics on Neurogenic Bladder
