Is Lymph Node Size a Reliable Factor for Estimating Lymph Node Metastasis in Early Gastric Cancer?
- Affiliations
-
- 1Department of Surgery, The Catholic University of Korea St. Paul's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea. djdjcap@catholic.ac.kr
- 2Department of Surgery, The Catholic University of Korea Yeouido St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea.
- KMID: 2414543
- DOI: http://doi.org/10.5230/jgc.2018.18.e1
Abstract
- PURPOSE
Pre-operative lymph node (LN) size is a valuable parameter for determining treatment strategy for gastric cancer. However, a correlation between LN size and metastasis has not been established.
MATERIALS AND METHODS
Thirty-six LN-positive (LNP) and matched 36 LN-negative (LNN) patients were included, and pathology slides of the LNs of these patients were reviewed. All the LNs were measured along the long-axis (LA) and short-axis (SA), manually.
RESULTS
Average retrieved LNs were 37.3±19.8 and 40.5±11.6 in the LNN and LNP groups, respectively. In total 2,800 LNs, including 136 metastatic LNs (MLNs) and 2,664 non-metastatic LNs (nMLNs), were evaluated. Mean length was significantly more in MLNs along both, the LA and SA (MLN_LA vs. nMLN_LA: 4.97±3.84 vs. 3.37±2.40 mm, MLN_SA vs. nMLN_SA: 3.86±3.19 vs. 2.43±1.59 mm; P<0.001). However, 92.6% (126/136) and 95.6% (130/136) of MLNs were <10 mm along the LA and SA, respectively. In addition, only 22.2% of the LNP group exhibited an MLN as the largest LN.
CONCLUSIONS
Pre-operative multi-detector computed tomography has limited ability in estimating the presence of metastasis in LNs because most MLNs are less than 10 mm, and only a small proportion of the LNP group exhibits an MLN as the largest MLN.
Keyword
Figure
-
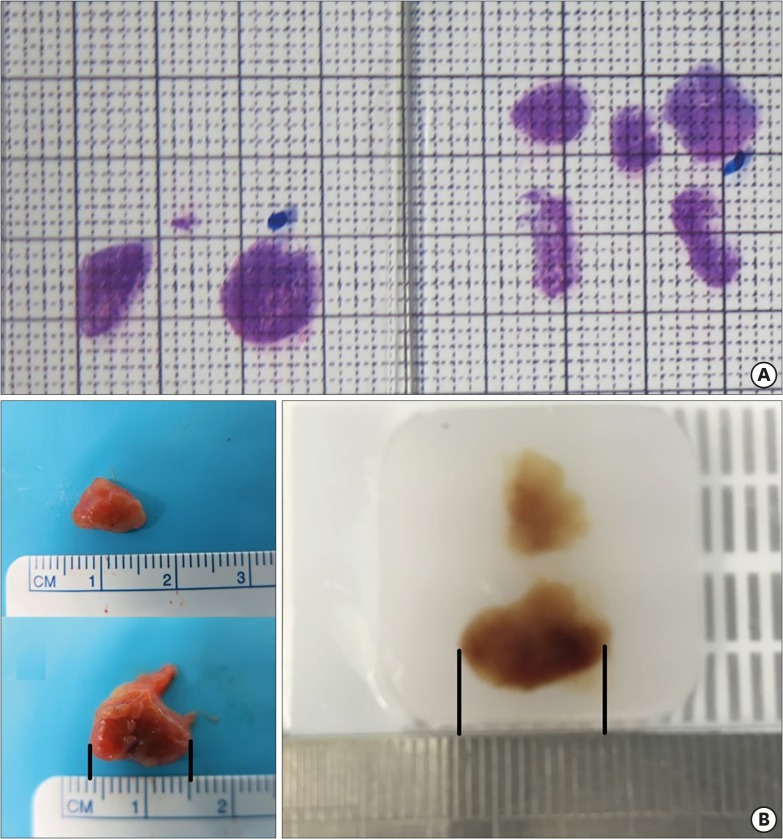
Fig. 1 (A) Representative photograph used for measuring LN size. (B) Comparison of LN size between a fresh specimen and a formalin-embedded specimen shows a minor size discrepancy (fresh vs. formalin-embedded, 11.0 vs. 10.5 mm).LN = lymph node.
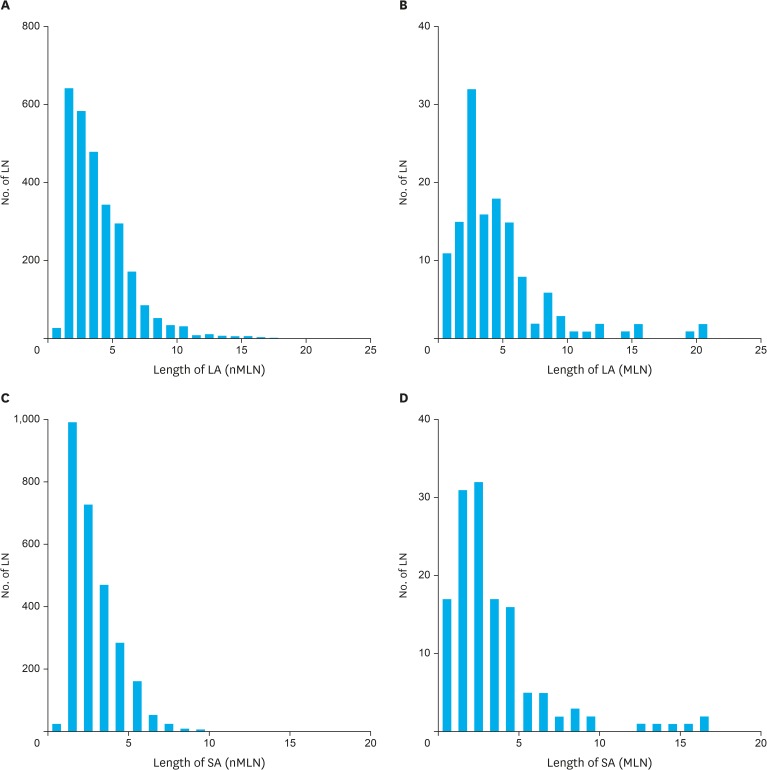
Fig. 2 Distribution of LN size according to (A) LA of nMLNs, (B) LA of MLNs, (C) SA of nMLNs (D) SA of MLNs.LN = lymph node; LA = long-axis; nMLN = non-metastatic lymph node; MLN = metastatic lymph node; SA = short-axis.
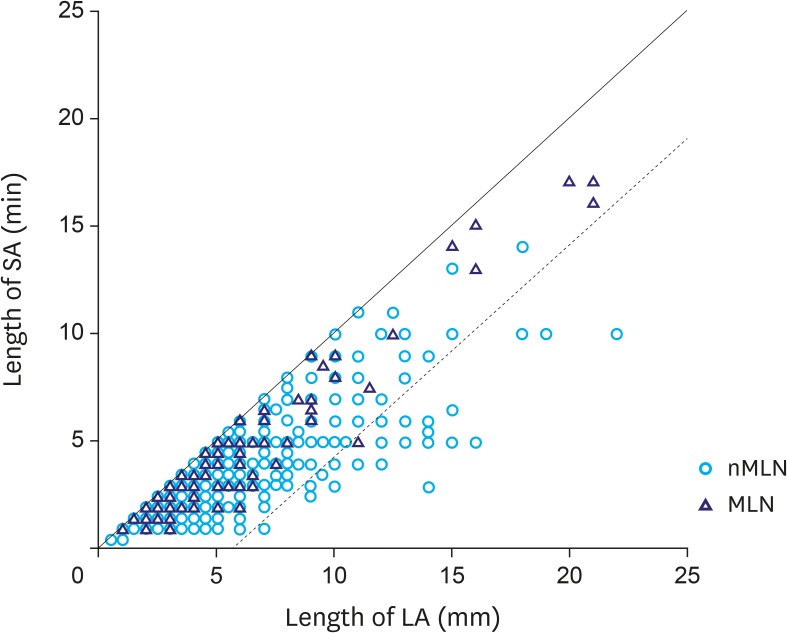
Fig. 3 Correlation between LA and SA of whole LNs (several circles are overlaid because of similar size).LA = long-axis; SA = short-axis; LN = lymph node; nMLN = non-metastatic lymph node; MLN = metastatic lymph node.
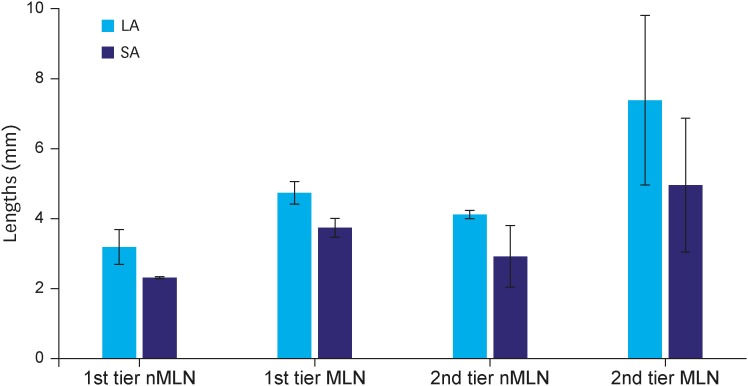
Fig. 4 Size difference according to LN stations.LN = lymph node; nMLN = non-metastatic lymph node; MLN = metastatic lymph node; LA = long-axis; SA = short-axis.
Reference
-
1. The Information Committee of the Korean Gastric Cancer Association. 2004 nationwide gastric cancer report in Korea. J Korean Gastric Cancer Assoc. 2007; 7:47–54.2. Jeong O, Park YK. Clinicopathological features and surgical treatment of gastric cancer in South Korea: the results of 2009 nationwide survey on surgically treated gastric cancer patients. J Gastric Cancer. 2011; 11:69–77. PMID: 22076206.
Article3. The Information Committee of Korean Gastric Cancer Association. Korean Gastric Cancer Association nationwide survey on gastric cancer in 2014. J Gastric Cancer. 2016; 16:131–140. PMID: 27752390.4. Nakamura K, Honda K, Akahoshi K, Ihara E, Matsuzaka H, Sumida Y, et al. Suitability of the expanded indication criteria for the treatment of early gastric cancer by endoscopic submucosal dissection: Japanese multicenter large-scale retrospective analysis of short- and long-term outcomes. Scand J Gastroenterol. 2015; 50:413–422. PMID: 25635364.
Article5. Kim YI, Kim YW, Choi IJ, Kim CG, Lee JY, Cho SJ, et al. Long-term survival after endoscopic resection versus surgery in early gastric cancers. Endoscopy. 2015; 47:293–301. PMID: 25625697.
Article6. Eom BW, Kim YI, Kim KH, Yoon HM, Cho SJ, Lee JY, et al. Survival benefit of additional surgery after noncurative endoscopic resection in patients with early gastric cancer. Gastrointest Endosc. 2017; 85:155–163.e3. PMID: 27460389.
Article7. Hirasawa T, Gotoda T, Miyata S, Kato Y, Shimoda T, Taniguchi H, et al. Incidence of lymph node metastasis and the feasibility of endoscopic resection for undifferentiated-type early gastric cancer. Gastric Cancer. 2009; 12:148–152. PMID: 19890694.
Article8. Kang HJ, Kim DH, Jeon TY, Lee SH, Shin N, Chae SH, et al. Lymph node metastasis from intestinal-type early gastric cancer: experience in a single institution and reassessment of the extended criteria for endoscopic submucosal dissection. Gastrointest Endosc. 2010; 72:508–515. PMID: 20554277.
Article9. Ahn HS, Lee HJ, Yoo MW, Kim SG, Im JP, Kim SH, et al. Diagnostic accuracy of T and N stages with endoscopy, stomach protocol CT, and endoscopic ultrasonography in early gastric cancer. J Surg Oncol. 2009; 99:20–27. PMID: 18937292.
Article10. Lee SL, Lee HH, Ku YM, Jeon HM. Usefulness of two-dimensional values measured using preoperative multidetector computed tomography in predicting lymph node metastasis of gastric cancer. Ann Surg Oncol. 2015; 22(Suppl 3):S786–S793. PMID: 25986871.
Article11. Tokunaga M, Sugisawa N, Tanizawa Y, Bando E, Kawamura T, Terashima M. The impact of preoperative lymph node size on long-term outcome following curative gastrectomy for gastric cancer. Ann Surg Oncol. 2013; 20:1598–1603. PMID: 23117474.
Article12. Yan C, Zhu ZG, Yan M, Zhang H, Pan ZL, Chen J, et al. Size of the largest lymph node visualized on multi-detector-row computed tomography (MDCT) is useful in predicting metastatic lymph node status of gastric cancer. J Int Med Res. 2010; 38:22–33. PMID: 20233510.
Article13. Xu J, Cao H, Yang JY, Suh YS, Kong SH, Kim SH, et al. Is preoperative staging enough to guide lymph node dissection in clinically early gastric cancer? Gastric Cancer. 2016; 19:568–578. PMID: 26231352.
Article14. Zhang Y, Zhu Z, Sun Z, Wang Z, Zheng X, Xu H. Preoperative predicting score of lymph node metastasis for gastric cancer. Tumour Biol. 2014; 35:10437–10442. PMID: 25053600.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Significance of Lymph Node Metastasis in Early Gastric Cancer
- Risk Factors Affecting Lymph Node Metastasis and Recurrence in Early Gastric Cancer
- Correlation Between Expression of p53, Bcl-2 Protein and Ki-67 Labelling Index and Lymph Node Metastasis in Early Gastric Cancer
- A Clinical Analysis of Recurrence and Lymphatic Metastasis in Early Gastric Cancer
- Analysis of Factors Related to Lymph Node Metastasis in Early Gastric Cancers
