Endoscope-Assisted Cochlear Implantation
- Affiliations
-
- 1Department of Otorhinolaryngology, Dokuz Eylül University School of Medicine, Izmir, Turkey. yuksel.olgun@deu.edu.tr
- KMID: 2412665
- DOI: http://doi.org/10.21053/ceo.2017.00927
Abstract
OBJECTIVES
Our aim was to present our endoscope-assisted cochlear implantation (CI) technique, in which the middle ear landmarks were identified through the facial recess exposure by using an endoscopic view without elevating the tympanic annulus. The secondary goal was to assess whether the situation of difficult surgical exposure could be predicted by evaluating preoperative axial computed tomography (CT) examinations.
METHODS
CT examinations and surgical outcomes of endoscope-assisted CI surgeries were analyzed.
RESULTS
A total of 179 CI operations performed in 27 adults (15.1%) and 152 children (84.9%) were retrospectively evaluated. It was found that in 14 cases (7.8%), endoscopic examination contributed substantially in identifying the round window (RW) membrane correctly. Endoscopic identification of the RW through the posterior tympanotomy enabled us to perform a straightforward surgery in all these cases, without the need for switching to a bony cochleostomy or alternative surgical techniques. The difficulty in the surgical exposure was predicted preoperatively by examining the axial CT scans in six of the 14 cases (42.8%) for which endoscopic assistance was necessary in order to identify the RW correctly.
CONCLUSION
The main benefit of endoscope-assisted CI is the improved visibility leading to a panoramic view of the RW region. The implementation of transfacial recess endoscopic examination into the conventional CI technique is helpful to avoid problems during surgical orientation. However, the difficulty in the surgical exposure of the RW cannot be reliably predicted by the subjective evaluation of preoperative CT scans and more studies are needed to obtain reliable criteria.
Keyword
MeSH Terms
Figure
-

Fig. 1. Adequate microscopical exposure of the round window region through posterior tympanotomy (right ear). Stapedial tendon, posterior crus of the stapes, incudostapedial joint and round window region are clearly visualized (A). Inadequate microscopical exposure of the round window region through posterior tympanotomy (facial recess approach, right ear). Round window region can not be visualized through the window delineated by chorda tympani laterally, facial nerve medially and the short process of incus cranially. The incudostapedial joint, umbo can be noticed (B). The round window niche could not be fully exposed in spite of a maximally opened proper posterior tympanotomy window (Saint Thomas Hospital classification type IIb) (C).

Fig. 2. Endoscopic view of the round window through the facial recess obtained with a 0º, 4 mm rigid endoscope before (A) and after (B) removing the round window niche (right ear).

Fig. 3. Endoscopic view of the round window (RW) region obtained with a 0º, 4 mm rigid endoscope inserted through the facial recess (right ear). RW region (A), RW membrane after removing the niche (B), membranous cochleostomy (C), electrode insertion (D).

Fig. 4. The first parameter used to determine the adequacy of the exposure: the depth of the region between the mastoid segment of the facial nerve and the round window on an axial computed tomography scan was evaluated in order to assess whether the facial recess approach would provide an adequate exposure (right ear; arrow points to the round window, arrowhead points to the mastoid segment of the facial nerve).
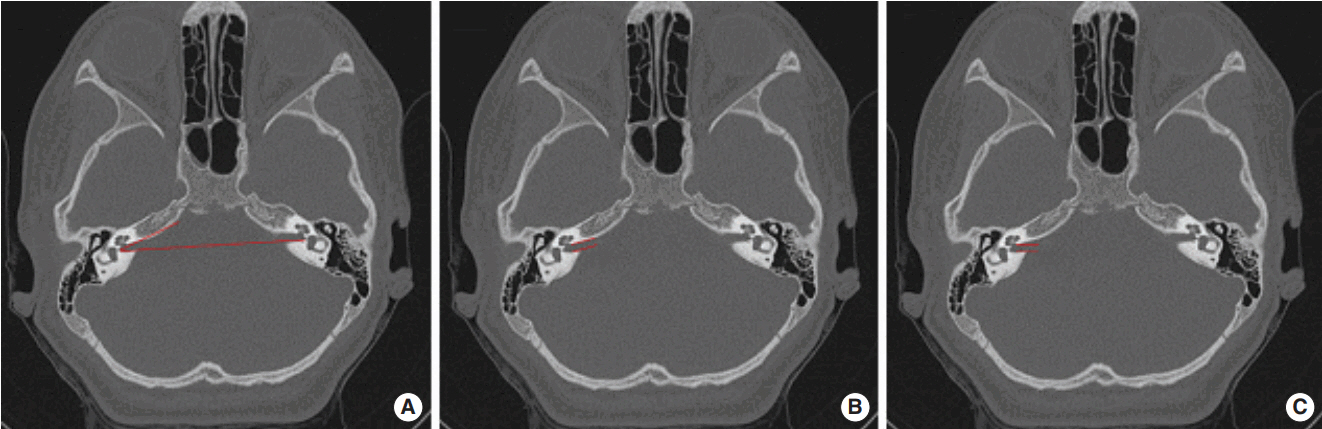
Fig. 5. The second parameter used to determine the adequacy of the exposure: the angle between the long axis of the IAC and a horizontal line drawn between the posterior borders of both internal auditory canals (IACs). (A) The angle is markedly increased on the right side and the IAC is inclined significantly anteriorly. (B) The IAC is nearly in horizontal orientation on the left side in comparison to (A). The expected orientation of the right IAC in relation to the location of the cochlea is illustrated in (C) (axial computed tomography scan).
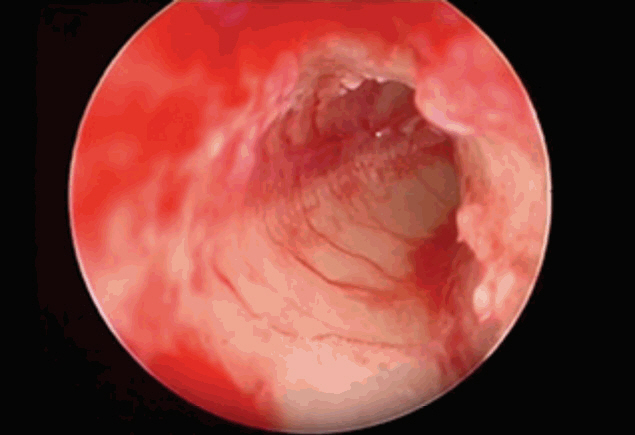
Fig. 6. Rigid endoscopic view (0º, 2.7 mm) of the scala tympani and modiolus (left ear).
Reference
-
1. House WF. Cochlear implants. Ann Otol Rhinol Laryngol. 1976; May-Jun. 85 suppl 27(3Pt2):1–93.
Article2. Terry B, Kelt RE, Jeyakumar A. Delayed complications after cochlear implantation. JAMA Otolaryngol Head Neck Surg. 2015; Nov. 141(11):1012–7.
Article3. Olgun Y, Bayrak AF, Catli T, Ceylan ME, Aydin R, Duzenli U, et al. Pediatric cochlear implant revision surgery and reimplantation: an analysis of 957 cases. Int J Pediatr Otorhinolaryngol. 2014; Oct. 78(10):1642–7.
Article4. Tarkan O, Tuncer U, Ozdemir S, Surmelioglu O, Cetik F, Kiroglu M, et al. Surgical and medical management for complications in 475 consecutive pediatric cochlear implantations. Int J Pediatr Otorhinolaryngol. 2013; Apr. 77(4):473–9.5. Loundon N, Blanchard M, Roger G, Denoyelle F, Garabedian EN. Medical and surgical complications in pediatric cochlear implantation. Arch Otolaryngol Head Neck Surg. 2010; Jan. 136(1):12–5.
Article6. Bibas A, Phillips S, Bailey CM, Papsin BC. Chronic suppurative otitis media following paediatric cochlear implantation. Cochlear Implants Int. 2006; Sep. 7(3):167–78.
Article7. Colletti V, Fiorino FG, Carner M, Pacini L. Basal turn cochleostomy via the middle fossa route for cochlear implant insertion. Am J Otol. 1998; Nov. 19(6):778–84.8. Kronenberg J, Migirov L, Dagan T. Suprameatal approach: new surgical approach for cochlear implantation. J Laryngol Otol. 2001; Apr. 115(4):283–5.
Article9. Kiratzidis T, Arnold W, Iliades T. Veria operation updated. I. The transcanal wall cochlear implantation. ORL J Otorhinolaryngol Relat Spec. 2002; Nov-Dec. 64(6):406–12.10. Hausler R. Cochlear implantation without mastoidectomy: the pericanal electrode insertion technique. Acta Otolaryngol. 2002; Oct. 122(7):715–9.11. Huang CC, Lin CY, Wu JL. Retrofacial approach of cochlear implantation in inner ear malformation with aberrant facial nerve: a case report. Auris Nasus Larynx. 2006; Jun. 33(2):179–82.
Article12. Sennaroglu L, Aydin E. Anteroposterior approach with split ear canal for cochlear implantation in severe malformations. Otol Neurotol. 2002; Jan. 23(1):39–42.13. Warren FM, Balachandran R, Fitzpatrick JM, Labadie RF. Percutaneous cochlear access using bone-mounted, customized drill guides: demonstration of concept in vitro. Otol Neurotol. 2007; Apr. 28(3):325–9.14. Carfrae MJ, Foyt D. Intact meatal skin, canal wall down approach for difficult cochlear implantation. J Laryngol Otol. 2009; Aug. 123(8):903–6.
Article15. Guneri EA. Endoscopic cochlear implantation procedures. Turk Klin J Ear Nose Throat. 2016; Mar. 9(1):46–51.16. Slavutsky V, Nicenboim L. Preliminary results in cochlear implant surgery without antromastoidectomy and with atraumatic electrode insertion: the endomeatal approach. Eur Arch Otorhinolaryngol. 2009; Apr. 266(4):481–8.
Article17. Lavinsky L, Lavinsky-Wolff M, Lavinsky J. Transcanal cochleostomy in cochlear implantation: experience with 50 cases. Cochlear Implants Int. 2010; Dec. 11(4):228–32.18. Kiumehr S, Mahboubi H, Middlebrooks JC, Djalilian HR. Transcanal approach for implantation of a cochlear nerve electrode array. Laryngoscope. 2013; May. 123(5):1261–5.
Article19. Marchioni D, Grammatica A, Alicandri-Ciufelli M, Genovese E, Presutti L. Endoscopic cochlear implant procedure. Eur Arch Otorhinolaryngol. 2014; May. 271(5):959–66.
Article20. Dia A, Nogueira JF, O’Grady KM, Redleaf M. Report of endoscopic cochlear implantation. Otol Neurotol. 2014; Dec. 35(10):1755–8.
Article21. Franz BK, Clark GM, Bloom DM. Surgical anatomy of the round window with special reference to cochlear implantation. J Laryngol Otol. 1987; Feb. 101(2):97–102.
Article22. Dahm MC, Shepherd RK, Clark GM. The postnatal growth of the temporal bone and its implications for cochlear implantation in children. Acta Otolaryngol Suppl. 1993; 505:1–39.
Article23. Leong AC, Jiang D, Agger A, Fitzgerald-O’Connor A. Evaluation of round window accessibility to cochlear implant insertion. Eur Arch Otorhinolaryngol. 2013; Mar. 270(4):1237–42.
Article24. Kashio A, Sakamoto T, Karino S, Kakigi A, Iwasaki S, Yamasoba T. Predicting round window niche visibility via the facial recess using high-resolution computed tomography. Otol Neurotol. 2015; Jan. 36(1):e18–23.
Article25. Fouad YA, Elaassar AS, El-Anwar MW, Sabir E, Abdelhamid A, Ghonimy M. Role of multislice CT imaging in predicting the visibility of the round window in pediatric cochlear implantation. Otol Neurotol. 2017; Sep. 38(8):1097–103.
Article26. Marchioni D, Soloperto D, Colleselli E, Tatti MF, Patel N, Jufas N. Round window chamber and fustis: endoscopic anatomy and surgical implications. Surg Radiol Anat. 2016; Nov. 38(9):1013–9.
Article27. Singla A, Sahni D, Gupta AK, Loukas M, Aggarwal A. Surgical anatomy of round window and its implications for cochlear implantation. Clin Anat. 2014; Apr. 27(3):331–6.
Article28. Meshik X, Holden TA, Chole RA, Hullar TE. Optimal cochlear implant insertion vectors. Otol Neurotol. 2010; Jan. 31(1):58–63.
Article29. Migirov L, Shapira Y, Wolf M. The feasibility of endoscopic transcanal approach for insertion of various cochlear electrodes: a pilot study. Eur Arch Otorhinolaryngol. 2015; Jul. 272(7):1637–41.
Article30. Hamamoto M, Murakami G, Kataura A. Topographical relationships among the facial nerve, chorda tympani nerve and round window with special reference to the approach route for cochlear implant surgery. Clin Anat. 2000; 13(4):251–6.
Article31. Tarabichi M, Nazhat O, Kassouma J, Najmi M. Endoscopic cochlear implantation: call for caution. Laryngoscope. 2016; Mar. 126(3):689–92.
Article32. Bruijnzeel H, Ziylan F, Cattani G, Grolman W, Topsakal V. Retrospective complication rate comparison between surgical techniques in paediatric cochlear implantation. Clin Otolaryngol. 2016; Dec. 41(6):666–72.
Article33. Marchioni D, Alicandri-Ciufelli M, Mattioli F, Nogeira JF, Tarabichi M, Villari D, et al. From external to internal auditory canal: surgical anatomy by an exclusive endoscopic approach. Eur Arch Otorhinolaryngol. 2013; Mar. 270(4):1267–75.
Article34. Tarabichi M, Kapadia M. Principles of endoscopic ear surgery. Curr Opin Otolaryngol Head Neck Surg. 2016; Oct. 24(5):382–7.
Article35. Labadie RF, Balachandran R, Noble JH, Blachon GS, Mitchell JE, Reda FA, et al. Minimally invasive image-guided cochlear implantation surgery: first report of clinical implementation. Laryngoscope. 2014; Aug. 124(8):1915–22.
Article36. Venail F, Bell B, Akkari M, Wimmer W, Williamson T, Gerber N, et al. Manual electrode array insertion through a robot-assisted minimal invasive cochleostomy: feasibility and comparison of two different electrode array subtypes. Otol Neurotol. 2015; Jul. 36(6):1015–22.37. Orhan KS, Polat B, Celik M, Comoglu S, Guldiken Y. Endoscopic-assisted cochlear implantation: a case series. J Int Adv Otol. 2016; Dec. 12(3):337–40.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cochlear Implantation
- Balance Problem after Cochlear Implantation
- Auditory Rehabilitation - Cochlear Implantation
- Cochlear Implant Failure due to Cochlear Nerve Deficiency in a Child with Normal Internal Auditory Canal
- Cochlear Implantation Using a Suprameatal Approach in a Case of Severely Contracted Mastoid Cavity
