Treatment of Late-Onset Legg-Calve-Perthes Disease by Arthrodiastasis
- Affiliations
-
- 1Department of Orthopaedic Surgery, Dong-A University College of Medicine, Busan, Korea. libi33@dau.ac.kr
- KMID: 2412329
- DOI: http://doi.org/10.4055/cios.2016.8.4.452
Abstract
- BACKGROUND
To evaluate the efficacy of arthrodiastasis for Legg-Calve-Perthes disease.
METHODS
Arthrodiastasis was conducted using external fixator devices (Orthofix) in 7 patients at least 8 years of age with a diagnosis of Legg-Calve-Perthes disease. The average follow-up was 80 months (range, 32 to 149 months), and their average age was 9.1 years (range, 8 to 12 years). The results of treatment were evaluated by measuring the degree of hip pain and the range of motion of the hip at 6 months after the operation and comparing the values with preoperative measurements. Radiological recovery was evaluated by the epiphyseal index and compared with the preoperative values. At the final follow-up, clinical and radiological results were evaluated using the Iowa hip score and the Stulberg classification.
RESULTS
On the clinical evaluation performed at 6 months after arthrodiastasis, the degree of pain decreased by 1.8 points on average, and the average flexion, internal rotation, and abduction increased by 35°, 16°, and 11°, respectively. Based on radiological findings, the epiphyseal index showed a remarkable increase of 6.6 on average (from 19 preoperatively to 26 postoperatively). At the final follow-up, the average Iowa hip score improved from 65 points preoperatively to 84 points. There were 1 Stulberg class I hip, 2 Stulberg class II hips, 3 Stulberg class III hips, 1 Stulberg class IV hip, and no Stulberg class V hip.
CONCLUSIONS
We conclude that arthrodiastasis using an external fixator can be a relatively promising surgical procedure for the treatment of late-onset Legg-Calve-Perthes disease.
Keyword
MeSH Terms
Figure
-
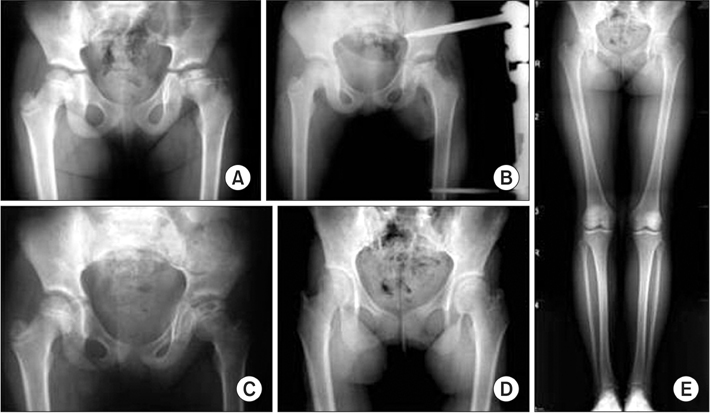
Fig. 1 (A) An 8-year-old girl shows left Legg-Calve-Perthes disease of Herring grade B on the radiograph. (B) Arthrodiastasis is performed. (C) Follow-up radiograph at 36 months after arthrodiastasis showing satisfactory femoral head regeneration. (D) Follow-up radiograph at 72 months after arthrodiastasis showing the reformed femoral head with congruency to the acetabulum. (E) Radiograph at the last follow-up (9 years) showing satisfactory results.

Fig. 2 (A) A 9-year-old boy shows right Legg-Calve-Perthes disease of Herring grade B on the radiograph. (B) Arthrodiastasis is performed. (C) Radiograph showing shortening of the femoral neck and relative overgrowth of the greater trochanter at 25 months after arthrodiastasis. (D) Greater trochanter distal transposition is done. (E) Shelf acetabuloplasty is performed for the coverage of femoral head at 94 months after arthrodiastasis. (F) Radiograph at the last follow-up (12 years) showing the reformed femoral head and the increased coverage of the femoral head with satisfactory clinical results.
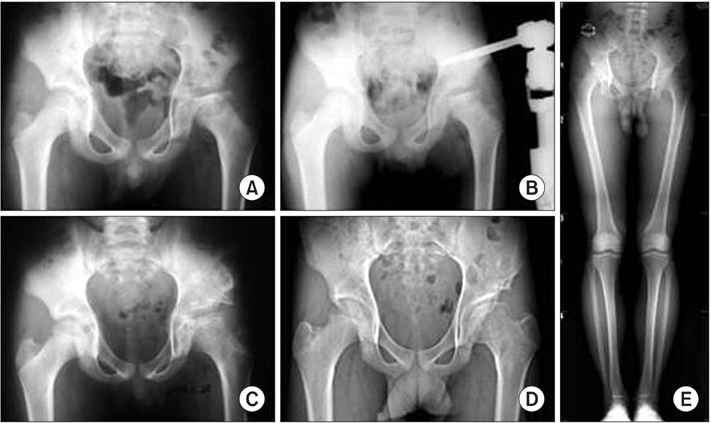
Fig. 3 (A) A 9-year-old boy shows left Legg-Calve-Perthes disease of Herring grade C on the radiograph. (B) Arthrodiastasis is performed. (C) Shelf osteotomy is done for the coverage of the femoral head at 28 months after arthrodiastasis. (D) Radiograph at 72 months after arthrodiastasis showing the increased coverage of the ovoid femoral head. (E) Radiograph at the last follow-up (7 years) showing relatively satisfactory results.
Reference
-
1. Stulberg SD, Cooperman DR, Wallensten R. The natural history of Legg-Calve-Perthes disease. J Bone Joint Surg Am. 1981; 63(7):1095–1108.2. Bellyei A, Mike G. Acetabular development in Legg-Calve-Perthes disease. Orthopedics. 1988; 11(3):407–411.3. Mazda K, Pennecot GF, Zeller R, Taussig G. Perthes' disease after the age of twelve years: role of the remaining growth. J Bone Joint Surg Br. 1999; 81(4):696–698.4. Herring JA, Kim HT, Browne R. Legg-Calve-Perthes disease. Part I: classification of radiographs with use of the modified lateral pillar and Stulberg classifications. J Bone Joint Surg Am. 2004; 86(10):2103–2120.5. Heyman CH, Herndon CH. Legg-Perthes disease: a method for the measurement of the roentgenographic result. J Bone Joint Surg Am. 1950; 32(4):767–778.6. Aldegheri R, Trivella G, Saleh M. Articulated distraction of the hip. In : De Bastiani G, Apley AG, Goldberg A, editors. Orthofix external fixation in trauma and orthopaedics. London: Springer Verlag;2000. p. 605–612.7. Aldegheri R, Trivella G, Saleh M. Articulated distraction of the hip: conservative surgery for arthritis in young patients. Clin Orthop Relat Res. 1994; (301):94–101.
Article8. Kocaoglu M, Kilicoglu OI, Goksan SB, Cakmak M. Ilizarov fixator for treatment of Legg-Calve-Perthes disease. J Pediatr Orthop B. 1999; 8(4):276–281.9. Guamiero R, Luzo CA, Montenegro NB, Godoy RM. Legg-Calve-Perthes disease: a comparative study between two types of treatment: femoral varus osteotomy and arthrochondrodiastasis with external fixation. In : 25th European Paediatric Ophthalmological Society (EPOS); 2000; Milan, Italy.10. Kucukkaya M, Kabukcuoglu Y, Ozturk I, Kuzgun U. Avascular necrosis of the femoral head in childhood: the results of treatment with articulated distraction method. J Pediatr Orthop. 2000; 20(6):722–728.
Article11. Daly K, Bruce C, Catterall A. Lateral shelf acetabuloplasty in Perthes' disease: a review of the end of growth. J Bone Joint Surg Br. 1999; 81(3):380–384.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Observation of the Legg-Calve-Perthes Disease: Preliminary Report
- Legg - Calve Perthes disease in Monozygotic Male Twins
- Osteochondritis Dissecans of Femoral Head Following Legg-Calve-Perthes Disease
- Innominate Osteotomy in Legg-Calve-Perthes Disease
- Late Complications of Legg-Calve-Perthes Disease
