Clin Orthop Surg.
2016 Dec;8(4):379-385. 10.4055/cios.2016.8.4.379.
Does Cruciate-Retaining Total Knee Arthroplasty Show Better Quadriceps Recovery than Posterior-Stabilized Total Knee Arthroplasty? - Objective Measurement with a Dynamometer in 102 Knees
- Affiliations
-
- 1Department of Medicine, Graduate School, Kyung Hee University, Seoul, Korea.
- 2Department of Orthopaedic Surgery, Center for Joint Diseases and Rheumatism, Kyung Hee University Hospital at Gangdong, Seoul, Korea. drkim@khu.ac.kr
- 3Department of Orthopaedic Surgery, College of Medicine, Kyung Hee University, Seoul, Korea.
- KMID: 2412319
- DOI: http://doi.org/10.4055/cios.2016.8.4.379
Abstract
- BACKGROUND
Cruciate-retaining (CR) prostheses have been considered to produce more physiologic femoral rollback, provide better proprioception, and result in better quadriceps recovery than posterior-stabilized (PS) prostheses after total knee arthroplasty (TKA). However, there are very few studies demonstrating these benefits in an objective manner. We investigated whether CR-TKA could result in (1) better quadriceps recovery; (2) a greater proportion of patients with beyond the preoperative level of recovery; and (3) better clinical outcomes than PS-TKA.
METHODS
This was a prospective non-randomized comparative study on the results of CR-TKA and PS-TKA. CR prostheses were used in 51 knees and PS prostheses in 51 knees. Quadriceps force was measured with a dynamometer preoperatively and at postoperative 6 weeks, 3 months, and 6 months consecutively. The Knee Society score (KSS) and range of motion (ROM) were also evaluated.
RESULTS
There were no differences between two groups in terms of the objective quadriceps force during the follow-up period. The proportion of patients with beyond the preoperative level of recovery was similar between groups. Moreover, the KSS and ROM were not significantly different between two groups.
CONCLUSIONS
CR-TKA did not result in better quadriceps recovery than PS-TKA during the 6-month follow-up. In other words, PS-TKA could lead to comparable quadriceps recovery despite greater preoperative weaknesses such as more restricted ROM and more severe degenerative changes of the knee.
MeSH Terms
Figure
-
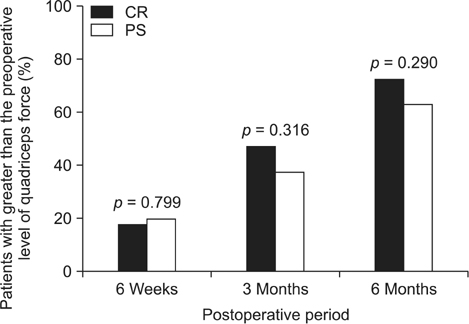
Fig. 1 Bar graph showing the proportion of patients with beyond the preoperative level of quadriceps force. CR: cruciate-retaining, PS: posterior-stabilized.
Reference
-
1. Andriacchi TP, Galante JO. Retention of the posterior cruciate in total knee arthroplasty. J Arthroplasty. 1988; 3 Suppl. S13–S19.
Article2. Dorr LD, Ochsner JL, Gronley J, Perry J. Functional comparison of posterior cruciate-retained versus cruciate-sacrificed total knee arthroplasty. Clin Orthop Relat Res. 1988; (236):36–43.3. Warren PJ, Olanlokun TK, Cobb AG, Bentley G. Proprioception after knee arthroplasty: the influence of prosthetic design. Clin Orthop Relat Res. 1993; (297):182–187.4. Simmons S, Lephart S, Rubash H, Borsa P, Barrack RL. Proprioception following total knee arthroplasty with and without the posterior cruciate ligament. J Arthroplasty. 1996; 11(7):763–768.
Article5. Swanik CB, Lephart SM, Rubash HE. Proprioception, kinesthesia, and balance after total knee arthroplasty with cruciate-retaining and posterior stabilized prostheses. J Bone Joint Surg Am. 2004; 86(2):328–334.
Article6. Berman AT, Bosacco SJ, Israelite C. Evaluation of total knee arthroplasty using isokinetic testing. Clin Orthop Relat Res. 1991; (271):106–113.
Article7. Bolanos AA, Colizza WA, McCann PD, et al. A comparison of isokinetic strength testing and gait analysis in patients with posterior cruciate-retaining and substituting knee arthroplasties. J Arthroplasty. 1998; 13(8):906–915.
Article8. Heyse TJ, Becher C, Kron N, et al. Quadriceps force in relation of intrinsic anteroposterior stability of TKA design. Arch Orthop Trauma Surg. 2010; 130(1):1–9.
Article9. Silva M, Shepherd EF, Jackson WO, Pratt JA, McClung CD, Schmalzried TP. Knee strength after total knee arthroplasty. J Arthroplasty. 2003; 18(5):605–611.
Article10. Tashiro Y, Miura H, Matsuda S, Okazaki K, Iwamoto Y. Minimally invasive versus standard approach in total knee arthroplasty. Clin Orthop Relat Res. 2007; 463:144–150.
Article11. Stevens-Lapsley JE, Balter JE, Kohrt WM, Eckhoff DG. Quadriceps and hamstrings muscle dysfunction after total knee arthroplasty. Clin Orthop Relat Res. 2010; 468(9):2460–2468.
Article12. Mizner RL, Petterson SC, Snyder-Mackler L. Quadriceps strength and the time course of functional recovery after total knee arthroplasty. J Orthop Sports Phys Ther. 2005; 35(7):424–436.
Article13. Clark CR, Rorabeck CH, MacDonald S, MacDonald D, Swafford J, Cleland D. Posterior-stabilized and cruciate-retaining total knee replacement: a randomized study. Clin Orthop Relat Res. 2001; (392):208–212.14. Conditt MA, Noble PC, Bertolusso R, Woody J, Parsley BS. The PCL significantly affects the functional outcome of total knee arthroplasty. J Arthroplasty. 2004; 19:7 Suppl 2. 107–112.
Article15. Lozano-Calderón SA, Shen J, Doumato DF, Greene DA, Zelicof SB. Cruciate-retaining vs posterior-substituting inserts in total knee arthroplasty: functional outcome comparison. J Arthroplasty. 2013; 28(2):234–242.e1.16. Andriacchi TP, Galante JO, Fermier RW. The influence of total knee-replacement design on walking and stair-climbing. J Bone Joint Surg Am. 1982; 64(9):1328–1335.
Article17. Parsley BS, Conditt MA, Bertolusso R, Noble PC. Posterior cruciate ligament substitution is not essential for excellent postoperative outcomes in total knee arthroplasty. J Arthroplasty. 2006; 21:6 Suppl 2. 127–131.
Article18. Insall JN, Lachiewicz PF, Burstein AH. The posterior stabilized condylar prosthesis: a modification of the total condylar design. Two to four-year clinical experience. J Bone Joint Surg Am. 1982; 64(9):1317–1323.19. Dennis DA, Komistek RD, Mahfouz MR. In vivo fluoroscopic analysis of fixed-bearing total knee replacements. Clin Orthop Relat Res. 2003; (410):114–130.
Article20. Dennis DA, Komistek RD, Mahfouz MR, Haas BD, Stiehl JB. Multicenter determination of in vivo kinematics after total knee arthroplasty. Clin Orthop Relat Res. 2003; (416):37–57.21. Dennis DA, Komistek RD, Hoff WA, Gabriel SM. In vivo knee kinematics derived using an inverse perspective technique. Clin Orthop Relat Res. 1996; (331):107–117.
Article22. Matsuda S, Whiteside LA, White SE, McCarthy DS. Knee kinematics of posterior cruciate ligament sacrificed total knee arthroplasty. Clin Orthop Relat Res. 1997; (341):257–266.
Article23. Bercik MJ, Joshi A, Parvizi J. Posterior cruciate-retaining versus posterior-stabilized total knee arthroplasty: a meta-analysis. J Arthroplasty. 2013; 28(3):439–444.
Article24. Witvrouw E, Victor J, Bellemans J, et al. A correlation study of objective functionality and WOMAC in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2002; 10(6):347–351.
Article25. Rooks DS, Huang J, Bierbaum BE, et al. Effect of preoperative exercise on measures of functional status in men and women undergoing total hip and knee arthroplasty. Arthritis Rheum. 2006; 55(5):700–708.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Postoperative Range of Motion and Functional Outcomes after Cruciate-Retaining and Posterior-Stabilized High-Flexion Total Knee Arthroplasty
- Posterior Cruciate Ligament Retaining Total Knee Arthroplasty
- Results of Posterior Cruciate Retaining and Cruciate Substituting Total Knee Arthroplasty (3 to 8 years follow up)
- Comparison of Posterior Cruciate Retaining & Substituting Total Knee Arthroplasty in Varus Deformity of Knee
- Is Single-Radius Design Better for Quadriceps Recovery in Total Knee Arthroplasty?
