Supplementary Technique for Unstable Clavicle Shaft Fractures: Interfragmentary Wiring and Temporary Axial K-Wire Pinning
- Affiliations
-
- 1Department of Orthopedic Surgery, CHA Gumi Medical Center, CHA University School of Medicine, Gumi, Korea. Kimykun83@gmail.com
- KMID: 2411738
- DOI: http://doi.org/10.4055/cios.2018.10.2.142
Abstract
- BACKGROUND
Treatment of unstable clavicle fractures remains a challenge for orthopedic surgeons, but the evolution of treatment strategies has allowed for reliable results with minimal complications. Although several surgical options exist, open reduction with plating remains the treatment of choice for clavicle fractures. The purpose of this study is to determine an easy way to achieve successful preplating reduction while minimizing surrounding soft tissue damage during treatment of midshaft fractures of the clavicle.
METHODS
A retrospective study included all consecutive adult patients operated on by a single surgeon for acute displaced clavicular midshaft fracture between January 2010 and October 2014. Hybrid technique with interfragmentary cerclage wiring, temporary axial K-wire pinning, or their combination was used in all patients. The demographic data and clinical outcomes, including operation time, union time, restoration of anatomy, shoulder functional score, and complications were evaluated.
RESULTS
There were 54 male and 19 female patients, with an average age of 39.3 years (range, 18 to 77 years) for males and 58.3 years (range, 39 to 77 years) for females. They were followed up for 24 months (range, 12 to 44 months). All patients had reliable bone union after surgery using interfragmentary cerclage wiring and temporary axial K-wire fixation; fracture union was obtained at an average of 11.7 weeks (range, 8 to 21 weeks) postoperatively. Additionally, there was no postoperative loss of fracture reduction or plate loosening. At the final follow-up, all patients had regained excellent functional outcomes.
CONCLUSIONS
The cognizant effort to achieve anatomic reduction without surrounding soft tissue insult before definitive plating allows excellent radiologic and functional outcomes. Interfragmentary cerclage wiring and temporary axial K-wire pinning can overcome difficulties associated with unstable clavicle fractures to allow proper fracture reduction. In this article, we introduce a concise technique for achieving the desired outcomes reliably and efficiently when treating unstable clavicle midshaft fractures.
Keyword
MeSH Terms
Figure
-
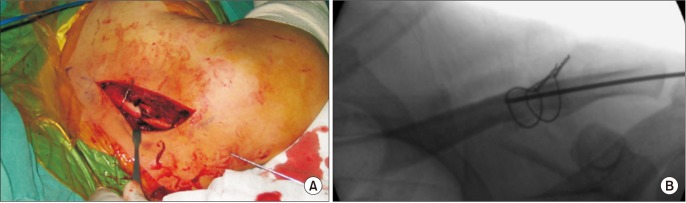
Fig. 1 (A) An unstable clavicle fracture with displaced, wedge-shaped fragments reduced with the combined technique of interfragmentary cerclage wiring and temporary axial K-wire pinning. The temporary axial K-wire penetrated the posterior cortex of the lateral curve. (B) Fluoroscopic image showing satisfactory reduction.
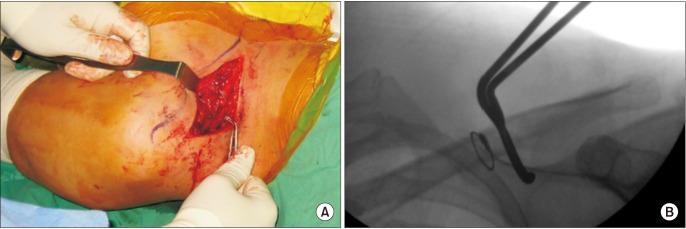
Fig. 2 (A) A wire passer was used to deliver thin wires under the fracture fragment with the surrounding soft tissue. Significant care was taken to minimize soft tissue injury. (B) Fluoroscopic image showing the position of the wire passer.
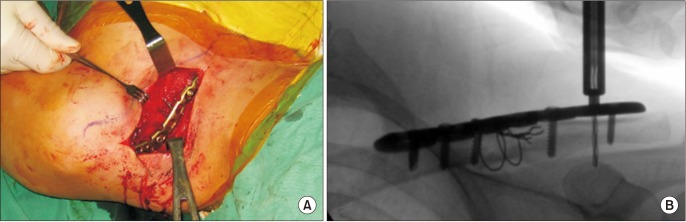
Fig. 3 (A) The cerclage wires between the clavicle and the anatomical plate were not obstacles for proper plate placement. (B) Fluoroscopic image showing the position of the wires and plate.
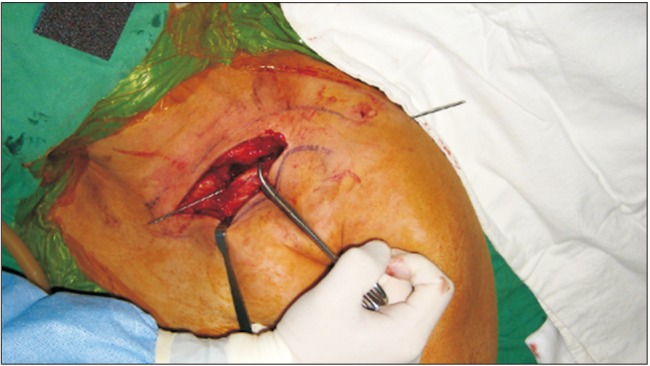
Fig. 4 The K-wire was retracted from the lateral fracture fragment through the skin until the medial end of K-wire reached the medial end of the lateral fracture fragment. After the fracture was reduced, the K-wire was further advanced into the medial fracture fragment.
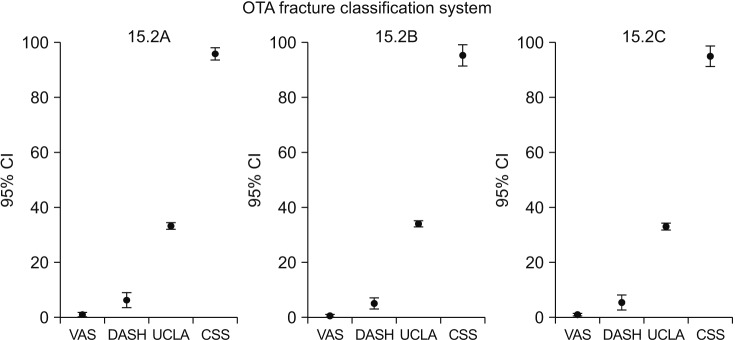
Fig. 5 Error bar graphs showing the functional results. The subgroups' clinical scores showed no statistically significant difference (p > 0.05). The error bars indicate 95% confidence intervals (CIs). OTA: Orthopedic Trauma Association, VAS: visual analogue scale, DASH: Disabilities of the Arm, Shoulder, and Hand, UCLA: University of California at Los Angeles Shoulder Score, CSS: Constant VAS DASH UCLA CSS Shoulder Score.
Reference
-
1. McKee RC, Whelan DB, Schemitsch EH, McKee MD. Operative versus nonoperative care of displaced midshaft clavicular fractures: a meta-analysis of randomized clinical trials. J Bone Joint Surg Am. 2012; 94(8):675–684. PMID: 22419410.
Article2. Nowak J, Holgersson M, Larsson S. Sequelae from clavicular fractures are common: a prospective study of 222 patients. Acta Orthop. 2005; 76(4):496–502. PMID: 16195064.3. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg. 2002; 11(5):452–456. PMID: 12378163.
Article4. NEER CS 2nd. Nonunion of the clavicle. J Am Med Assoc. 1960; 172(10):1006–1011. PMID: 14426324.
Article5. Rowe CR. An atlas of anatomy and treatment of midclavicular fractures. Clin Orthop Relat Res. 1968; 58:29–42. PMID: 5666865.6. Hill JM, McGuire MH, Crosby LA. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br. 1997; 79(4):537–539. PMID: 9250733.
Article7. Jeray KJ. Acute midshaft clavicular fracture. J Am Acad Orthop Surg. 2007; 15(4):239–248. PMID: 17426295.
Article8. Wijdicks FJ, Van der, Millett PJ, Verleisdonk EJ, Houwert RM. Systematic review of the complications of plate fixation of clavicle fractures. Arch Orthop Trauma Surg. 2012; 132(5):617–625. PMID: 22237694.
Article9. Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures: a multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007; 89(1):1–10.10. Lenza M, Belloti JC, Andriolo RB, Faloppa F. Conservative interventions for treating middle third clavicle fractures in adolescents and adults. Cochrane Database Syst Rev. 2014; (5):CD007121. PMID: 24879341.
Article11. Smekal V, Oberladstaetter J, Struve P, Krappinger D. Shaft fractures of the clavicle: current concepts. Arch Orthop Trauma Surg. 2009; 129(6):807–815. PMID: 18989685.
Article12. van der Ven Denise JC, Timmers TK, Flikweert PE, Van Ijseldijk AL, van Olden GD. Plate fixation versus conservative treatment of displaced midshaft clavicle fractures: functional outcome and patients' satisfaction during a mean follow-up of 5 years. Injury. 2015; 46(11):2223–2229. PMID: 26315667.
Article13. Robinson CM, Goudie EB, Murray IR, et al. Open reduction and plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: a multicenter, randomized, controlled trial. J Bone Joint Surg Am. 2013; 95(17):1576–1584. PMID: 24005198.14. Golish SR, Oliviero JA, Francke EI, Miller MD. A biomechanical study of plate versus intramedullary devices for midshaft clavicle fixation. J Orthop Surg Res. 2008; 3:28. PMID: 18631380.
Article15. Naderipour A, McKee MD. Precontoured plate fixation with interfragmentary lag screw use in a middle third clavicle fracture fixation. J Orthop Trauma. 2015; 7. 28. [Epub]. DOI: 10.1097/BOT.0000000000000402.
Article16. Bostman O, Manninen M, Pihlajamaki H. Complications of plate fixation in fresh displaced midclavicular fractures. J Trauma. 1997; 43(5):778–783. PMID: 9390489.
Article17. Stanley D, Trowbridge EA, Norris SH. The mechanism of clavicular fracture: a clinical and biomechanical analysis. J Bone Joint Surg Br. 1988; 70(3):461–464. PMID: 3372571.
Article18. Yum JK, Shin YW, Lee HS, Park JG. Does interfragmentary cerclage wire fixation in clavicle shaft fracture interfere the fracture healing? J Korean Fract Soc. 2011; 24(2):138–143.
Article19. Celestre P, Roberston C, Mahar A, Oka R, Meunier M, Schwartz A. Biomechanical evaluation of clavicle fracture plating techniques: does a locking plate provide improved stability? J Orthop Trauma. 2008; 22(4):241–247. PMID: 18404033.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Additional fixation using a metal plate with bioresorbable screws and wires for robinson type 2B clavicle fracture
- Does Interfragmentary Cerclage Wire Fixation in Clavicle Shaft Fracture Interfere the Fracture Healing?
- Use of Composite Wiring on Surgical Treatments of Clavicle Shaft Fractures
- Intramedullary Fixation in the Fracture of the Shaft of the Clavicle by Threaded Kirschner Wire
- Strength of Surgical Wire by Different Wiring Technique
