Use of Composite Wiring on Surgical Treatments of Clavicle Shaft Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, Semyeong Christianty Hospital, Pohang, Korea. handkkim@naver.com
- KMID: 2344091
- DOI: http://doi.org/10.12671/jkfs.2016.29.3.185
Abstract
- PURPOSE
To introduce the technique of reducing displaced or comminuted clavicle shaft fracture using composite wiring and report the clinical results.
MATERIALS AND METHODS
Between March 2006 and December 2013, 31 consecutive displaced clavicle fractures (Edinburgh classification 2B) treated by anatomic reduction and internal fixation using composite wiring and plates were retrospectively evaluated. The fracture fragments were anatomically reduced and fixed with composite-wiring. An additional plate was applied. Radiographic assessments for the numbers of fragments, size of each fragment and amount of shortening and displacement were performed. The duration for fracture union and complications were investigated retrospectively. The mean fallow-up duration was 15.9 months.
RESULTS
The mean number of fragments was 1.7 (1-3) and the mean width of fracture fragment was 7.1 mm (4.5-10.6 mm). The mean shortening of the clavicle was 20.5 mm (10.3-36.2 mm). The mean number of composite wires used in fixation was 1.9 (1-3). Radiographic union was achieved in all patients with a mean time to union of 11.6 weeks. There were no complications including metal failure, pin migration, nonunion, or infection.
CONCLUSION
The composite wiring was suitable for fixation of small fracture fragment and did not interfere with the union, indicating that it is useful for treatment of clavicle shaft fracture.
Keyword
Figure
-

Fig. 1 The preoperative 3 dimensional-computed tomography shows segmental clavicle mid-shaft fractures (Edinburgh classification type 2B2).
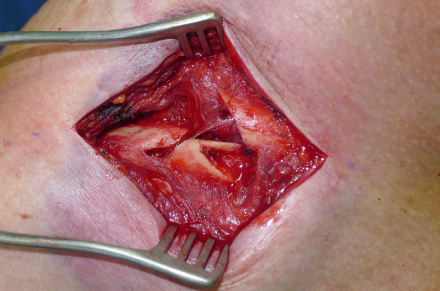
Fig. 2 Intraoperative photograph showing segmental clavicle mid-shaft fractures.
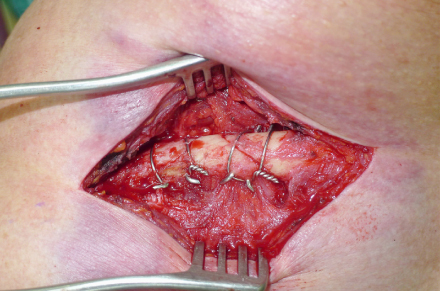
Fig. 3 The fracture fragments were reduced and fixed by two composite-wires with minimal soft tissue dissection.

Fig. 4 The fracture was fixed in an anatomical position with the reconstruction plate and screws.
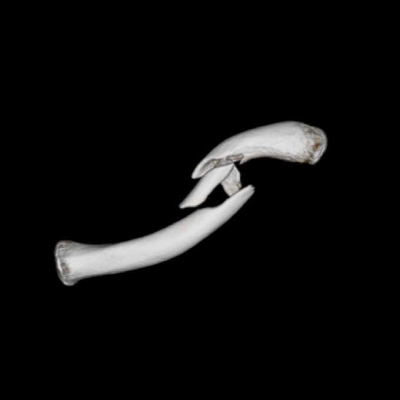
Fig. 5 The preoperative 3 dimensional-computed tomography shows segmental comminuted clavicle mid-shaft fractures (Edinburgh classification type 2B2).
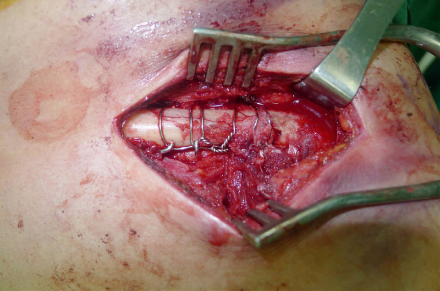
Fig. 6 The small fracture fragments were fixed by three composite-wiring.
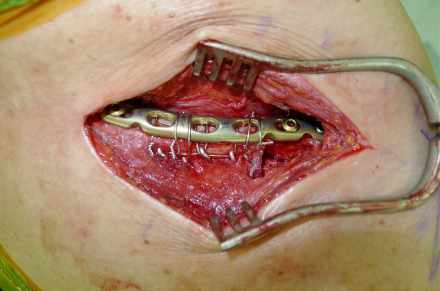
Fig. 7 Additional wiring over the plate was fixed to resist pull-out stress.
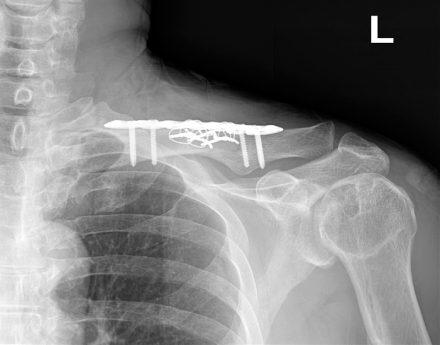
Fig. 8 The fracture was fixed in anatomical position with the reconstruction plate and screws.
Reference
-
1. Post M. Current concepts in the treatment of fractures of the clavicle. Clin Orthop Relat Res. 1989; (245):89–101.
Article2. Kim W, McKee MD. Management of acute clavicle fractures. Orthop Clin North Am. 2008; 39:491–505.
Article3. McKee MD, Pedersen EM, Jones C, et al. Deficits following nonoperative treatment of displaced midshaft clavicular fractures. J Bone Joint Surg Am. 2006; 88:35–40.
Article4. Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD. Evidence-Based Orthopaedic Trauma Working Group. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma. 2005; 19:504–507.
Article5. Khan LA, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg Am. 2009; 91:447–460.
Article6. van der Meijden OA, Gaskill TR, Millett PJ. Treatment of clavicle fractures: current concepts review. J Shoulder Elbow Surg. 2012; 21:423–429.
Article7. Andermahr J, Jubel A, Elsner A, et al. Anatomy of the clavicle and the intramedullary nailing of midclavicular fractures. Clin Anat. 2007; 20:48–56.
Article8. Huang JI, Toogood P, Chen MR, Wilber JH, Cooperman DR. Clavicular anatomy and the applicability of precontoured plates. J Bone Joint Surg Am. 2007; 89:2260–2265.
Article9. Shen WJ, Liu TJ, Shen YS. Plate fixation of fresh displaced midshaft clavicle fractures. Injury. 1999; 30:497–500.
Article10. Shin SJ, Do NH, Jang KY. Risk factors for postoperative complications of displaced clavicular midshaft fractures. J Trauma Acute Care Surg. 2012; 72:1046–1050.
Article11. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br. 1998; 80:476–484.12. Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc. 1960; 172:1006–1011.
Article13. Nowak J, Mallmin H, Larsson Larsson. The aetiology and epidemiology of clavicular fractures. A prospective study during a two-year period in Uppsala, Sweden. Injury. 2000; 31:353–358.
Article14. Koh KH, Shon MS, Lee SW, Kim JH, Yoo JC. Anatomical reduction of all fracture fragments and fixation using inter-fragmentary screw and plate in comminuted and displaced clavicle mid-shaft fracture. J Korean Fract Soc. 2012; 25:300–304.
Article15. Yum JK, Shin YW, Lee HS, Park JG. Does Interfragmentary cerclage wire fixation in clavicle shaft fracture interfere the fracture healing?. J Korean Fract Soc. 2011; 24:138–143.
Article16. Greene TL, Noellert RC, Belsole RJ. Treatment of unstable metacarpal and phalangeal fractures with tension band wiring techniques. Clin Orthop Relat Res. 1987; (214):78–84.
Article17. Flinkkilä T, Ristiniemi J, Hyvönen P, Hämäläinen M. Surgical treatment of unstable fractures of the distal clavicle: a comparative study of Kirschner wire and clavicular hook plate fixation. Acta Orthop Scand. 2002; 73:50–53.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Periprosthetic Clavicle Shaft Fracture After Treatment of Type V Distal Clavicle Fracture Using a Hook Plate: A Report of Two Cases
- Current concepts in the treatment of midshaft clavicle fractures in adults
- Does Interfragmentary Cerclage Wire Fixation in Clavicle Shaft Fracture Interfere the Fracture Healing?
- Current Concepts for Classification and Treatment of Distal Clavicle Fractures
- Mini-open Treatment Using Plate of Clavicle Mid-shaft Fractures
