Pelvic MRI: Is Endovaginal or Rectal Filling Needed?
- Affiliations
-
- 1Department of Radiology, Centre Hospitalo-Universitaire de Reims, Reims 51092, France. constance.e@hotmail.fr
- 2Department of Radiology, Centre Hospitalier de Valenciennes, Valenciennes 59300, France.
- 3Department of Abdominal Imaging, Hôpital Lariboisière-APHP, Paris 75010, France.
- 4Department of Radiology, Hospices civils de Lyon, Centre hospitalier Lyon-Sud, Université Claude-Bernard Lyon 1, Pierre-Bénite 69495, France.
- KMID: 2410810
- DOI: http://doi.org/10.3348/kjr.2018.19.3.397
Abstract
- Magnetic resonance imaging is the optimal modality for pelvic imaging. It is based on T2-weighted magnetic resonance (MR) sequences allowing uterine and vaginal cavity assessment as well as rectal evaluation. Anatomical depiction of these structures may benefit from distension, and conditions either developing inside the lumen of cavities or coming from the outside may then be better delineated and localized. The need for distension, either rectal or vaginal, and the way to conduct it are matters of debate, depending on indication for which the MR examination is being conducted. In this review, we discuss advantages and potential drawbacks of this technique, based on literature and our experience, in the evaluation of various gynecological and rectal diseases.
Keyword
Figure
-
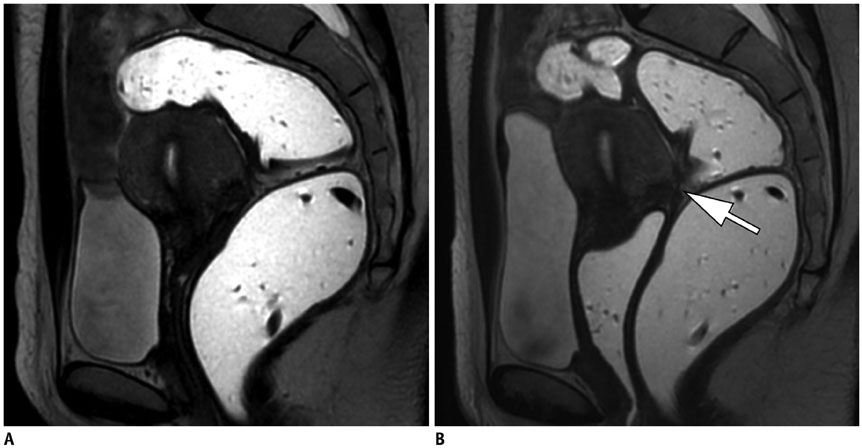
Fig. 1 30-year-old woman with clinical suspicion of endometriosis (dysmenorrhea). T2-weighted MR sequences in sagittal plane with rectal opacification only (A), and after rectal and vaginal opacification (B). Endometriotic nodule revealing low signal intensity is more conspicuous after vaginal distension (arrow) (B) than before use of opacification. Vaginal lesions are ruled out. MR = magnetic resonance
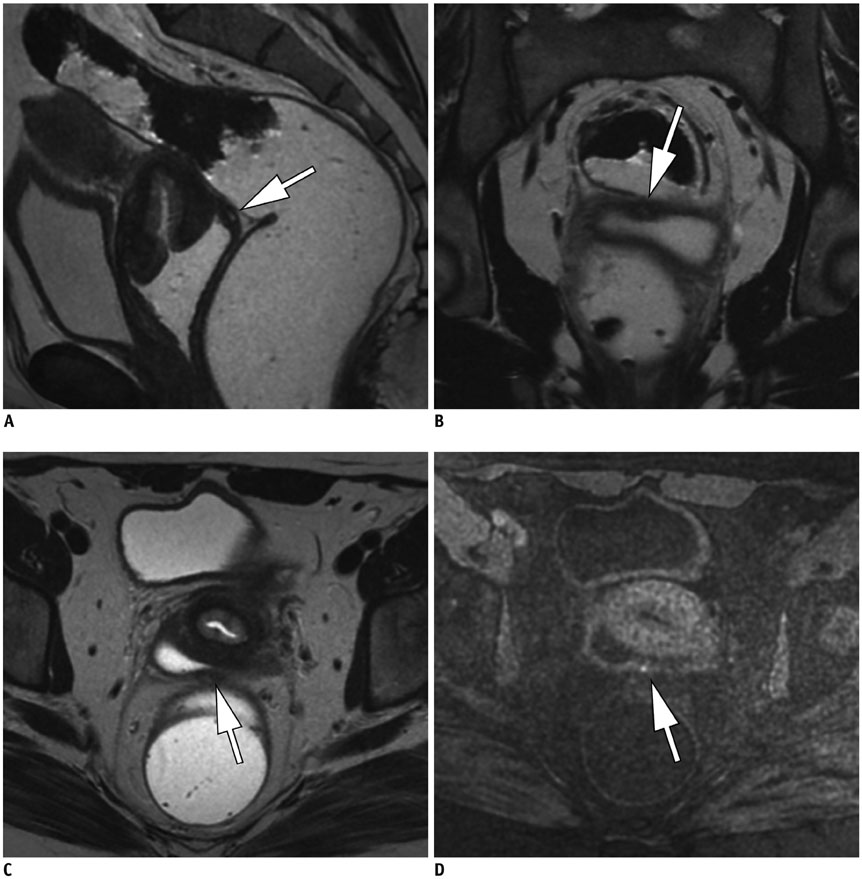
Fig. 2 Pelvic MRI study in 27-year-old female with endometriosis that presents dyspareunia. T2-weighted MR images with rectal and vaginal opacification in sagittal (A), coronal (B), and axial (C) planes. Thanks to vaginal distension, thin fibrous lesion in posterior vaginal fornix displaying low signal intensity on T2-weighted images (arrows) (A-C) and hemorrhagic microcyst displaying high signal intensity focus on fat-suppressed T1-weighted MR image (arrow) (D) are depicted. MRI = magnetic resonance imaging
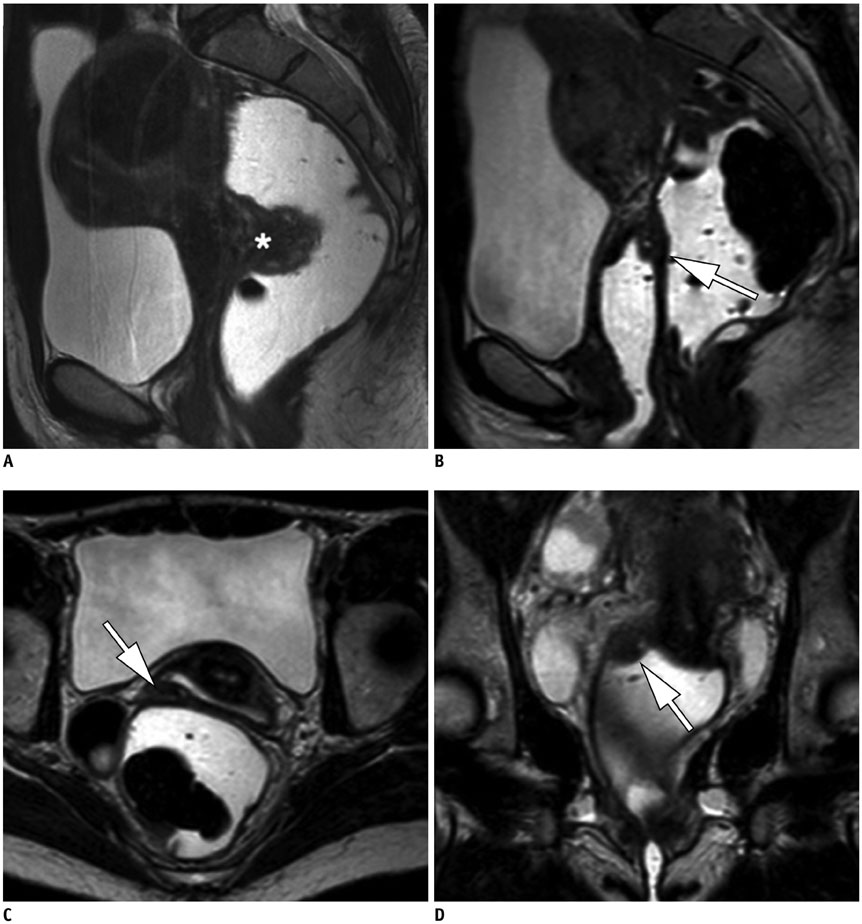
Fig. 3 Pre-operative MR images in 37-year-old patient with known endometriosis and suffering from recurrent dyschesia. Sagittal T2-weighted MR view with rectal opacification (A) revealing endometriotic nodule of anterior wall of rectum (*), surgically removed. MRI conducted after surgery using T2-weighted MR images after vaginal and rectal opacification in sagittal (B), axial (C), and coronal (D) planes demonstrates endometriotic nodule in lateral right vaginal fornix (arrows) (B-D). This lesion had not been detected on pre-operative MR imaging, probably because of absence of initial vaginal distension.
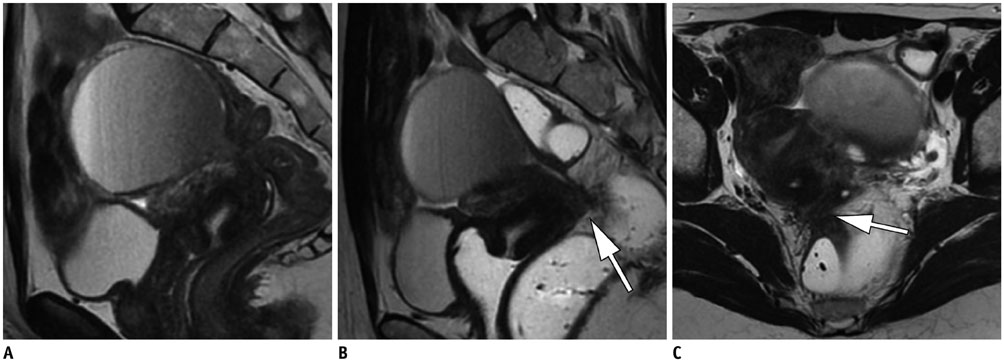
Fig. 4 Pre-operative pelvic MR study in 28-year-old female with endometriosis presenting pain radiating to back. Sagittal T2-weighted MR image using vaginal and rectal opacification reveals thick lesion in posterior vaginal fornix and posterior cervix (arrow) (B). There is large nodular lesion infiltrating anterior rectal wall on axial T2-weighted MR image (arrow) (C), associated with Douglas cul-de-sac obliteration. Vaginal and rectal opacification clearly improve detection of these lesions compared to what was observed on MR image MRI study conducted without opacification (A).

Fig. 5 Sagittal T2-weighted MR images without and after vaginal opacification in two women (respectively 41-year-old and 47-year-old) with cervical carcinoma. Relatively high signal-intensity tumor is observed in posterior cervix (arrow). Vaginal fornices appear to be invaded by mass in absence of vaginal distension (A). After vaginal opacification, borders of tumor are better observed, and no vaginal extension is depicted in second case (arrow) (B). Tumor′s boundaries are less conspicuous without opacification.

Fig. 6 45-year-old female with cervical tumor undergoing pretherapeutic MRI. Sagittal T2-weighted MR image reveals large cervical tumor (*). Vaginal opacification nicely delineates wellpreserved posterior vaginal wall (arrow).
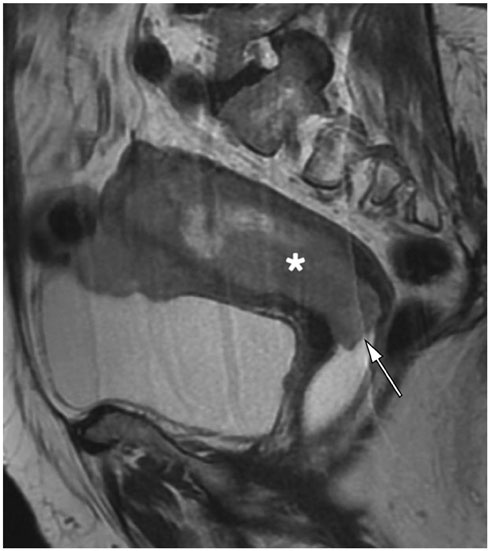
Fig. 7 67-year-old female with endometrial carcinoma (*). Sagittal T2-weighted MR image reveals that vaginal opacification facilitates identification of absence of vaginal involvement (arrow) from mass related to endometrial carcinoma (*).
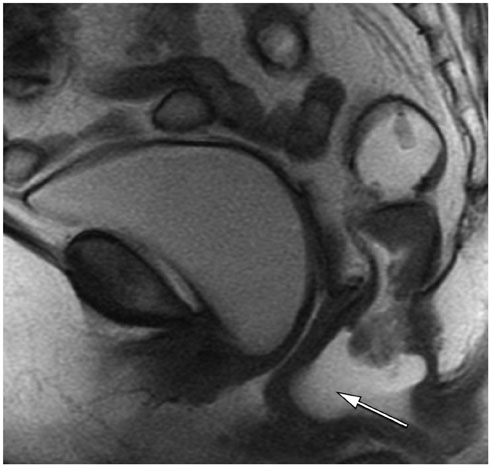
Fig. 8 Midsagittal T2-weighted MR image in 62-year-old patient with dyssynergic defecation. Distension of rectum simulates rectocele as rectal gel has not been completely evacuated during maximal straining (arrow).
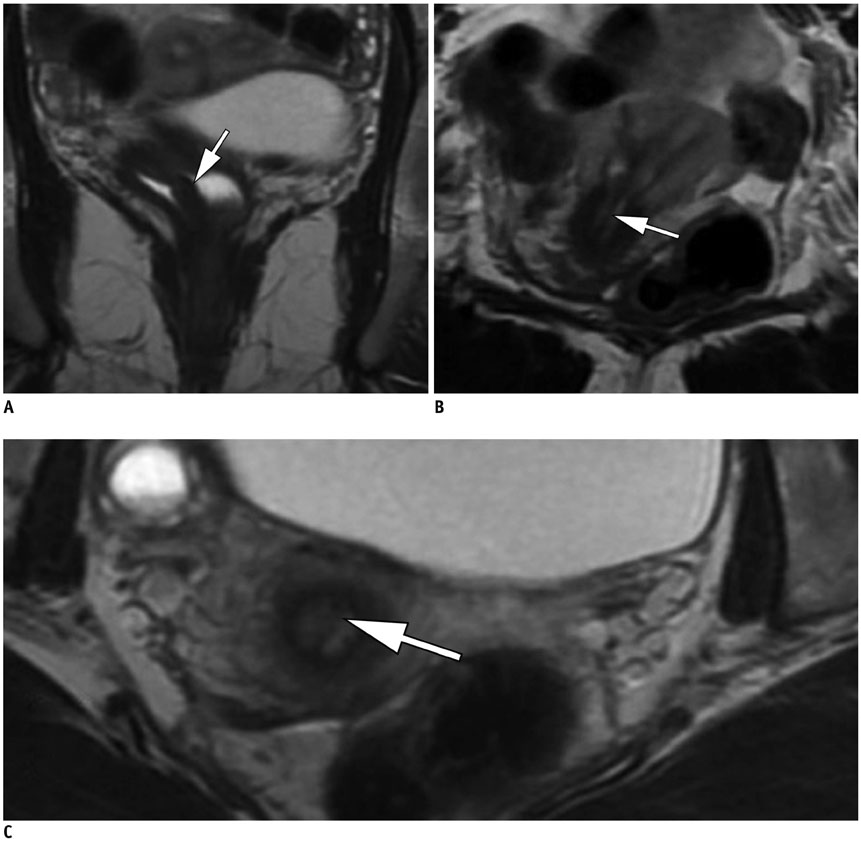
Fig. 9 27-year-old woman suffering from infertility. A. Coronal T2-weighted MR image with ultrasound gel vaginal opacification reveals septate vagina (arrow), outlined by high T2 signal intensity from ultrasound endovaginal gel. B, C. Axial T2-weighted MR images in same patient at different levels reveal complete septate uterus with septum displaying homogenous low signal T2 signal and extending from fundus to cervix (arrows).
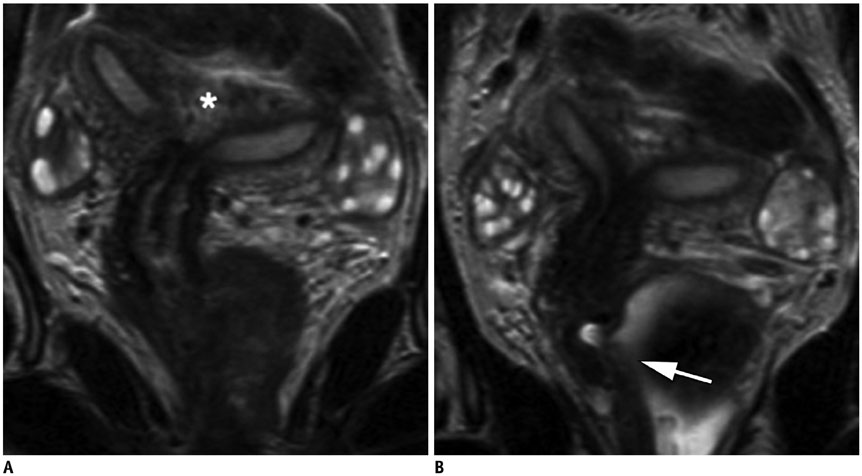
Fig. 10 25-year-old patient with story of recurrent spontaneous miscarriages. A. Coronal T2-weighted MR image without opacification image reveals bicornuate uterus with significant fundal cleft (*). B. Coronal T2-weighted MR images obtained with endovaginal gel reveal incomplete vaginal septation (arrow), easily overlooked without opacification.
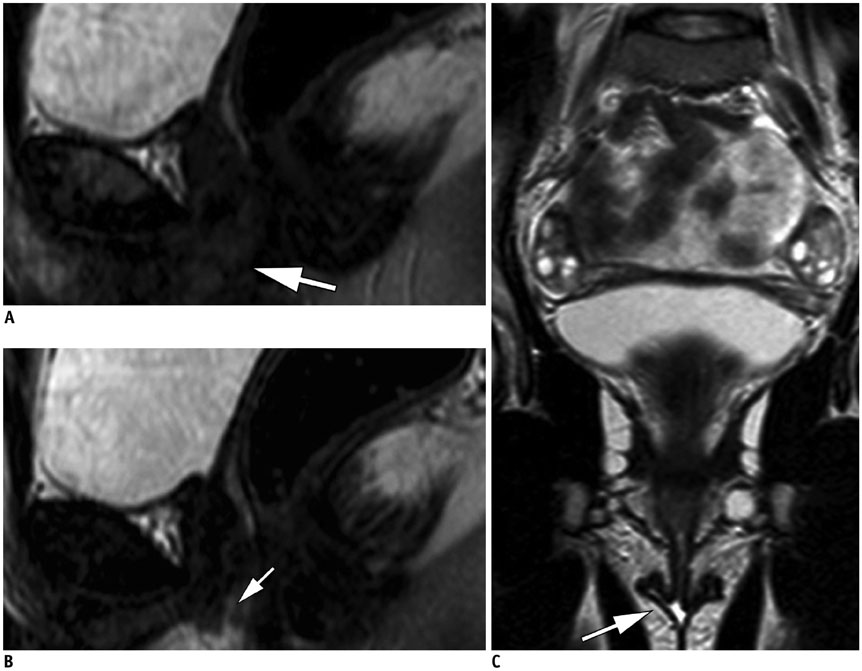
Fig. 11 18-year-old female with Mayer-Rokitansky-Küster-Hauser syndrome. Sagittal T2-weighted MR image reveals absence of uterus. Vagina is not observed (arrow) (A). After opacification, on sagittal (B) and coronal (C) T2-weighted MR image, gel is not observed inside vagina (hypoplasic vagina), but underlines labiae (arrows). Ovaries are normal.

Fig. 12 49-year-old woman complaining of mass in lower part of vagina. A. Vaginal abnormalities are observed in sagittal T2-weighted MR images without vaginal opacification, but are difficult to analyze (arrow). B. After vaginal opacification was conducted subsequently, three cysts of anterior vaginal wall became much more conspicuous (arrows).
Reference
-
1. Lienemann A, Fischer T. Functional imaging of the pelvic floor. Eur J Radiol. 2003; 47:117–122.
Article2. Bitti GT, Argiolas GM, Ballicu N, Caddeo E, Cecconi M, Demurtas G, et al. Pelvic floor failure: MR imaging evaluation of anatomic and functional abnormalities. Radiographics. 2014; 34:429–448.
Article3. Marchiolè P, Cittadini G, Sala P, Moioli M, Mathevet P, Capaccio E, et al. Pre- and post-operative work-up in patients affected by early cervical cancer and eligible for fertilitysparing treatment: role of MRI with saline hydrocolpos. Abdom Imaging. 2010; 35:271–279.
Article4. Maccioni F. Functional disorders of the ano-rectal compartment of the pelvic floor: clinical and diagnostic value of dynamic MRI. Abdom Imaging. 2013; 38:930–951.
Article5. Hetzer FH, Andreisek G, Tsagari C, Sahrbacher U, Weishaupt D. MR defecography in patients with fecal incontinence: imaging findings and their effect on surgical management. Radiology. 2006; 240:449–457.
Article6. Reiner CS, Weishaupt D. Dynamic pelvic floor imaging: MRI techniques and imaging parameters. Abdom Imaging. 2013; 38:903–911.
Article7. Reiner CS, Tutuian R, Solopova AE, Pohl D, Marincek B, Weishaupt D. MR defecography in patients with dyssynergic defecation: spectrum of imaging findings and diagnostic value. Br J Radiol. 2011; 84:136–144.
Article8. Maas M, Lambregts DM, Lahaye MJ, Beets GL, Backes W, Vliegen RF, et al. T-staging of rectal cancer: accuracy of 3.0 Tesla MRI compared with 1.5 Tesla. Abdom Imaging. 2012; 37:475–481.9. Ye F, Zhang H, Liang X, Ouyang H, Zhao X, Zhou C. Journal club: preoperative MRI evaluation of primary rectal cancer: intrasubject comparison with and without rectal distention. AJR Am J Roentgenol. 2016; 207:32–39.
Article10. Fiaschetti V, Crusco S, Meschini A, Cama V, Di Vito L, Marziali M, et al. Deeply infiltrating endometriosis: evaluation of retro-cervical space on MRI after vaginal opacification. Eur J Radiol. 2012; 81:3638–3645.
Article11. Chassang M, Novellas S, Bloch-Marcotte C, Delotte J, Toullalan O, Bongain A, et al. Utility of vaginal and rectal contrast medium in MRI for the detection of deep pelvic endometriosis. Eur Radiol. 2010; 20:1003–1010.
Article12. Novellas S, Marcotte Bloch C, Berthier F, Fournol M, Delotte J, Bongain A, et al. [Anatomy of the female pelvis on MRI: value of intravaginal contrast]. J Radiol. 2009; 90(7-8 Pt 1):819–824.13. Bazot M, Gasner A, Lafont C, Ballester M, Dara E. Deep pelvic endometriosis: limited additional diagnostic value of postcontrast in comparison with conventional MR images. Eur J Radiol. 2011; 80:331–339.
Article14. Macario S, Chassang M, Novellas S, Baudin G, Delotte J, Toullalan O, et al. The value of pelvic MRI in the diagnosis of posterior cul-de-sac obliteration in cases of deep pelvic endometriosis. AJR Am J Roentgenol. 2012; 199:1410–1415.
Article15. Chami LP, Blasbalg R, Pereira RM, Warmbrand G, Serafini PC. Findings of pelvic endometriosis at transvaginal US, MR imaging, and laparoscopy. Radiographics. 2011; 31:77–100.
Article16. Takeuchi H, Kuwatsuru R, Kitade M, Sakurai A, Kikuchi I, Shimanuki H, et al. A novel technique using magnetic resonance imaging jelly for evaluation of rectovaginal endometriosis. Fertil Steril. 2005; 83:442–447.
Article17. Kikuchi I, Kuwatsuru R, Yamazaki K, Kumakiri J, Aoki Y, Takeda S. Evaluation of the usefulness of the MRI jelly method for diagnosing complete cul-de-sac obliteration. Biomed Res Int. 2014; 2014:437962.
Article18. Loubeyre P, Copercini M, Frossard JL, Wenger JM, Petignat P. Pictorial review: rectosigmoid endometriosis on MRI with gel opacification after rectosigmoid colon cleansing. Clin Imaging. 2012; 36:295–300.
Article19. Bazot M, Bharwani N, Huchon C, Kinkel K, Cunha TM, Guerra A, et al. European society of urogenital radiology (ESUR) guidelines: MR imaging of pelvic endometriosis. Eur Radiol. 2017; 27:2765–2775.
Article20. Coutinho A Jr, Bittencourt LK, Pires CE, Junqueira F, Lima CM, Coutinho E, et al. MR imaging in deep pelvic endometriosis: a pictorial essay. Radiographics. 2011; 31:549–567.
Article21. Brown MA, Mattrey RF, Stamato S, Sirlin CB. MRI of the female pelvis using vaginal gel. AJR Am J Roentgenol. 2005; 185:1221–1227.
Article22. El Sayed RF, Alt CD, Maccioni F, Meissnitzer M, Masselli G, Manganaro L, et al. Magnetic resonance imaging of pelvic floor dysfunction - joint recommendations of the ESUR and ESGAR pelvic floor working group. Eur Radiol. 2017; 27:2067–2085.
Article23. Colaiacomo MC, Masselli G, Polettini E, Lanciotti S, Casciani E, Bertini L, et al. Dynamic MR imaging of the pelvic floor: a pictorial review. Radiographics. 2009; 29:e35.
Article24. Khatri G, Bailey AA, Bacsu C, Christie AL, Kumar N, Pedrosa I, et al. Influence of rectal gel volume on defecation during dynamic pelvic floor magnetic resonance imaging. Clin Imaging. 2015; 39:1027–1031.
Article25. Francesca M, Najwa AA, Valeria B, Fabrizio M, Marileda I, Massimo M, et al. Prospective comparison between two different magnetic resonance defecography techniques for evaluating pelvic floor disorders: air-balloon versus gel for rectal filling. Eur Radiol. 2016; 26:1783–1791.
Article26. García del Salto L, de Miguel Criado J, Aguilera del Hoyo LF, Gutiérrez Velasco L, Fraga Rivas P, Manzano Paradela M, et al. MR imaging-based assessment of the female pelvic floor. Radiographics. 2014; 34:1417–1439.
Article27. Lienemann A, Anthuber C, Baron A, Kohz P, Reiser M. Dynamic MR colpocystorectography assessing pelvic-floor descent. Eur Radiol. 1997; 7:1309–1317.
Article28. Hoeffel C, Mulé S, Laurent V, Bouché O, Volet J, Soyer P. Primary rectal cancer local staging. Diagn Interv Imaging. 2014; 95:485–494.
Article29. Loubeyre P, Petignat P, Jacob S, Egger JF, Dubuisson JB, Wenger JM. Anatomic distribution of posterior deeply infiltrating endometriosis on MRI after vaginal and rectal gel opacification. AJR Am J Roentgenol. 2009; 192:1625–1631.
Article30. Hottat N, Larrousse C, Anaf V, Noël J-C, Matos C, Absil J, et al. Endometriosis: contribution of 3.0-T pelvic MR imaging in preoperative assessment--initial results. Radiology. 2009; 253:126–134.
Article31. Balleyguier C, Sala E, Da Cunha T, Bergman A, Brkljacic B, Danza F, et al. Staging of uterine cervical cancer with MRI: guidelines of the European Society of Urogenital Radiology. Eur Radiol. 2011; 21:1102–1110.
Article32. Akata D, Kerimoglu U, Hazirolan T, Karcaaltincaba M, Köse F, Ozmen MN, et al. Efficacy of transvaginal contrast-enhanced MRI in the early staging of cervical carcinoma. Eur Radiol. 2005; 15:1727–1733.
Article33. Young P, Daniel B, Sommer G, Kim B, Herfkens R. Intravaginal gel for staging of female pelvic cancers--preliminary report of safety, distention, and gel-mucosal contrast during magnetic resonance examination. J Comput Assist Tomogr. 2012; 36:253–256.
Article34. Mondot L, Novellas S, Senni M, Piche T, Dausse F, Caramella T, et al. Pelvic prolapse: static and dynamic MRI. Abdom Imaging. 2007; 32:775–783.
Article35. Chan YY, Jayaprakasan K, Zamora J, Thornton JG, Raine-Fenning N, Coomarasamy A. The prevalence of congenital uterine anomalies in unselected and high-risk populations: a systematic review. Hum Reprod Update. 2011; 17:761–771.
Article36. Troiano RN, McCarthy SM. Mullerian duct anomalies: imaging and clinical issues. Radiology. 2004; 233:19–34.37. Griffin N, Grant LA, Sala E. Magnetic resonance imaging of vaginal and vulval pathology. Eur Radiol. 2008; 18:1269–1280.
Article38. Yoo RE, Cho JY, Kim SY, Kim SH. A systematic approach to the magnetic resonance imaging-based differential diagnosis of congenital Müllerian duct anomalies and their mimics. Abdom Imaging. 2015; 40:192–206.
Article39. Beets-Tan RG, Lambregts DM, Maas M, Bipat S, Barbaro B, Caseiro-Alves F, et al. Magnetic resonance imaging for the clinical management of rectal cancer patients: recommendations from the 2012 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. 2013; 23:2522–2531.
Article40. Slater A, Halligan S, Taylor SA, Marshall M. Distance between the rectal wall and mesorectal fascia measured by MRI: effect of rectal distension and implications for preoperative prediction of a tumour-free circumferential resection margin. Clin Radiol. 2006; 61:65–70.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preoperative Evaluation of Lower Rectal Cancer by Pelvic MR with and without Gel Filling
- Interpretation of Rectal MRI after Neoadjuvant Treatment in Patients with Rectal Cancer
- Clinical Implication of Lateral Pelvic Lymph Node Metastasis in Rectal Cancer Treated with Neoadjuvant Chemoradiotherapy
- The efficacy of MRI to diagnosis the bladder and rectal invasion in cervical cancer
- Rectal Injury Associated with Pelvic Fracture
