Can recording only the day-time voided volumes predict bladder capacity?
- Affiliations
-
- 1Department of Urology, Dong-A University College of Medicine, Busan, Korea.
- 2Department of Urology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. H00181@paik.ac.kr
- 3Department of Urology, Chonnam National University Medical School, Gwangju, Korea.
- 4Department of Urology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- 5Department of Urology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 6Department of Urology, Chung-Ang University College of Medicine, Seoul, Korea.
- 7Department of Urology, Korea University College of Medicine, Seoul, Korea.
- 8Department of Urology, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- 9Department of Urology, Soonchunhyang University Bucheon Hospital, Bucheon, Korea.
- KMID: 2410593
- DOI: http://doi.org/10.4111/icu.2018.59.3.194
Abstract
- PURPOSE
This study aimed to demonstrate a method to easily assess bladder capacity using knowledge of day-time voided volumes, which can be obtained even from patients with nocturnal enuresis where the first morning void cannot accurately predict the bladder capacity due to bladder emptying overnight.
MATERIALS AND METHODS
We evaluated 177 healthy children from 7 Korean medical centres entered the study between January 2008 and January 2009. Voided volumes measured for more than 48 hours were recorded in the frequency volume chart (FVC).
RESULTS
Most voided volumes during day-time were showed between 30% and 80% of the maximal voided volume (MVV). The maximal voided volume during day-time (MVVDT) was significantly less than the MVV (179.5±71.1 mL vs. 227.0±79.2 mL, p < 0.001). The correlation coefficients with the MVV were 0.801 for the estimated MVV using the MVVDT (MVVDT×1.25), which suggested a fairly strong relationship between the MVVDT×1.25 and the MVV.
CONCLUSIONS
The MVV derived from the FVC excluding the FMV was less than if the FMV had been included. When an accurate first morning voided volume cannot be obtained, as in patients with nocturnal enuresis, calculating MVVDT×1.25 allows estimation of the bladder capacity in place of the MVV.
Keyword
Figure
-
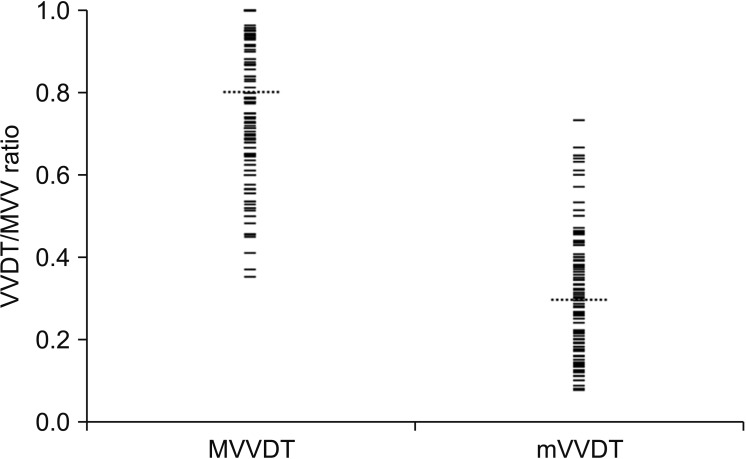
Fig. 1 Scatter plots of the MVVDT/MVV (Rmax) and mVVDT/MVV (Rmin) ratios. The mean Rmax was 0.80±0.17 (0.35–1.00) and mean Rmin was 0.30±0.15 (0.08–0.73). MVV, maximal voided volume; VVDT, voided volume during day-time; MVVDT, maximal VVDT; mVVDT, minimal VVDT.
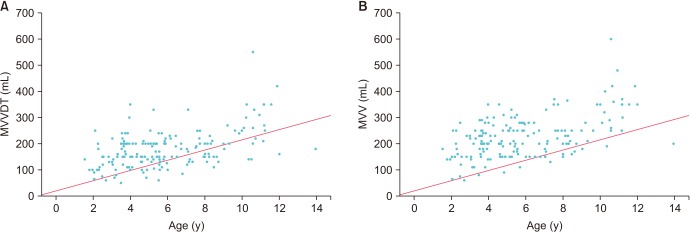
Fig. 2 Scatter plots of the maximal voided volume during day-time (MVVDT) and the maximal voided volume (MVV) versus age. The dotted line is the limit below which children are considered to have decreased bladder capacity compared to estimated bladder capacity for their age (y=0.65×30×(age+1)). (A) While 22.0% of the data points are below the line in the MVVDT vs. age plot, (B) 7.3% are below the line in the MVV vs. age plot.
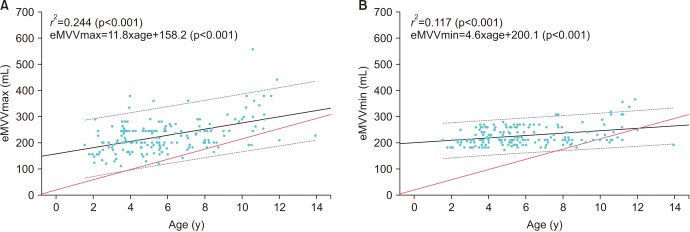
Fig. 3 The estimated maximal voided volume using the maximal voided volume during day-time (MVVDT) and the minimal voided volume during the day-time (mVVDT) eMVVmax (A) and eMVVmin (B) plotted versus age, with 5% and 95% reference ranges (dotted grey lines). Y=0.65×30×(age+1) (thin solid line).
Reference
-
1. Rushton HG, Belman AB, Zaontz MR, Skoog SJ, Sihelnik S. The influence of small functional bladder capacity and other predictors on the response to desmopressin in the management of monosymptomatic nocturnal enuresis. J Urol. 1996; 156:651–655. PMID: 8683752.2. Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al. The standardisation of terminology of lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Neurourol Urodyn. 2002; 21:167–178. PMID: 11857671.
Article3. Mattsson S, Gladh G, Lindström S. Relative filling of the bladder at daytime voids in healthy school children. J Urol. 2003; 170:1343–1346. PMID: 14501766.
Article4. Rittig S, Kamperis K, Siggaard C, Hagstroem S, Djurhuus JC. Age related nocturnal urine volume and maximum voided volume in healthy children: reappraisal of International Children's Continence Society definitions. J Urol. 2010; 183:1561–1567. PMID: 20176383.
Article5. Van Hoeck K, Bael A, Lax H, Hirche H, Van Dessel E, Van Renthergem D, et al. Urine output rate and maximum volume voided in school-age children with and without nocturnal enuresis. J Pediatr. 2007; 151:575–580. PMID: 18035133.
Article6. Van Hoeck K, Bael A, Lax H, Hirche H, van Gool JD. Circadian variation of voided volume in normal school-age children. Eur J Pediatr. 2007; 166:579–584. PMID: 17043843.
Article7. Martínez-García R, Ubeda-Sansano MI, Díez-Domingo J, Pérez-Hoyos S, Gil-Salom M. It is time to abandon "expected bladder capacity." Systematic review and new models for children's normal maximum voided volumes. Neurourol Urodyn. 2014; 33:1092–1098. PMID: 23847007.
Article8. Mattsson SH. Voiding frequency, volumes and intervals in healthy schoolchildren. Scand J Urol Nephrol. 1994; 28:1–11. PMID: 8009180.
Article9. Hjalmas K, Arnold T, Bower W, Caione P, Chiozza LM, von Gontard A, et al. Nocturnal enuresis: an international evidence based management strategy. J Urol. 2004; 171:2545–2561.
Article10. Kim SO, Kim KD, Kim YS, Kim JM, Moon du G, Park S, et al. Evaluation of maximum voided volume in Korean children by use of a 48-h frequency volume chart. BJU Int. 2012; 110:597–600. PMID: 22145861.
Article11. Radvanska E, Kovács L, Rittig S. The role of bladder capacity in antidiuretic and anticholinergic treatment for nocturnal enuresis. J Urol. 2006; 176:764–768. discussion 768-9. PMID: 16813940.
Article12. Tauris LH, Kamperis K, Hagstroem S, Bower WF, Rittig S. Tailoring treatment of monosymptomatic nocturnal enuresis: the role of maximum voided capacity. J Urol. 2012; 187:664–669. PMID: 22177206.
Article13. Graugaard-Jensen C, Schmidt F, Thomsen HF, Djurhuus JC. Normal voiding patterns assessed by means of a frequency-volume chart. Scand J Urol Nephrol. 2008; 42:269–273. PMID: 18432534.
Article14. Kawauchi A, Tanaka Y, Naito Y, Yamao Y, Ukimura O, Yoneda K, et al. Bladder capacity at the time of enuresis. Urology. 2003; 61:1016–1018. PMID: 12736027.
Article15. Hagstroem S, Kamperis K, Rittig S, Djurhuus JC. Bladder reservoir function in children with monosymptomatic nocturnal enuresis and healthy controls. J Urol. 2006; 176:759–763. PMID: 16813939.
Article16. Hagstroem S, Kamperis K, Rittig S, Rijkhoff NJ, Djurhuus JC. Monosymptomatic nocturnal enuresis is associated with abnormal nocturnal bladder emptying. J Urol. 2004; 171:2562–2566. discussion 2566. PMID: 15118419.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of a Sonographic Bladder Scan for Uroflowmetry and the Evaluation of the Anxiety Level Associated with Uroflowmetry
- Age Related Changes of Voiding Patterns in Women with Overactive Bladder
- The Value of Urine Cytology in the Diagnosis and Follow-up of the Bladder Tumors
- Voiding Pattern in Healthy Korean Children Below 3 Years Old
- Evaluation of the NMP22 test and comparison with voided urine cytology in the detection of bladder cancer
