Re-establishment of occlusal plane in a patient with a failed implant prosthesis
- Affiliations
-
- 1Department of Prosthodontics and Research Institute of Oral Science, College of Dentistry, Gangneung-Wonju National University, Gangneung, Republic of Korea. doctorcj@gwnu.ac.kr
- KMID: 2410118
- DOI: http://doi.org/10.4047/jkap.2018.56.2.141
Abstract
- A non-physiological occlusal plane caused by continuous tooth loss, occlusal wear, and failure of a prosthesis may result in an unattractive appearance and functional problems, such as reduced masticatory efficiency and occlusal interference. Therefore, when undertaking prosthetic treatment for edentulous patients or patients with a collapsed occlusal plane, it is important to establish an occlusal plane that is compatible with masticatory function. The patient in this case report had undergone restoration of a completely edentulous maxilla using an implant-supported fixed prosthesis. On follow-up examination in the following 6 years, mechanical complications were observed in the existing implant prosthesis, including porcelain chipping, occlusal wear, and screw loosening. Moreover, due to occlusal wear and supraeruption of the opposing anterior teeth, as well as loss of some posterior teeth, the occlusal plane had collapsed. Following diagnosis, the patient underwent full mouth rehabilitation, involving additional implant installation in edentulous sites, recreation of the existing prosthesis, and prosthetic restoration of all remaining teeth.
MeSH Terms
Figure
-

Fig. 1. Intraoral examination in 6 years ago. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.

Fig. 2. Prosthetic rehabilitation in 6 years ago. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.

Fig. 3. (A) Horizontal root fracture of the mandibular right first premolar, (B) Vertical root fracture of the mandibular left first molar.

Fig. 4. Re-evaluation after 6 years of prothetic rehabilitation. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.

Fig. 5. Radiographic examination. Misfit between the abutment and the prosthesis.

Fig. 6. (A) Lateral cephalometric radiograph, (B) Transcranial radiograph. Hypermobility of the left condyle and no specific findings related with pathologic bony change in both TMJs.
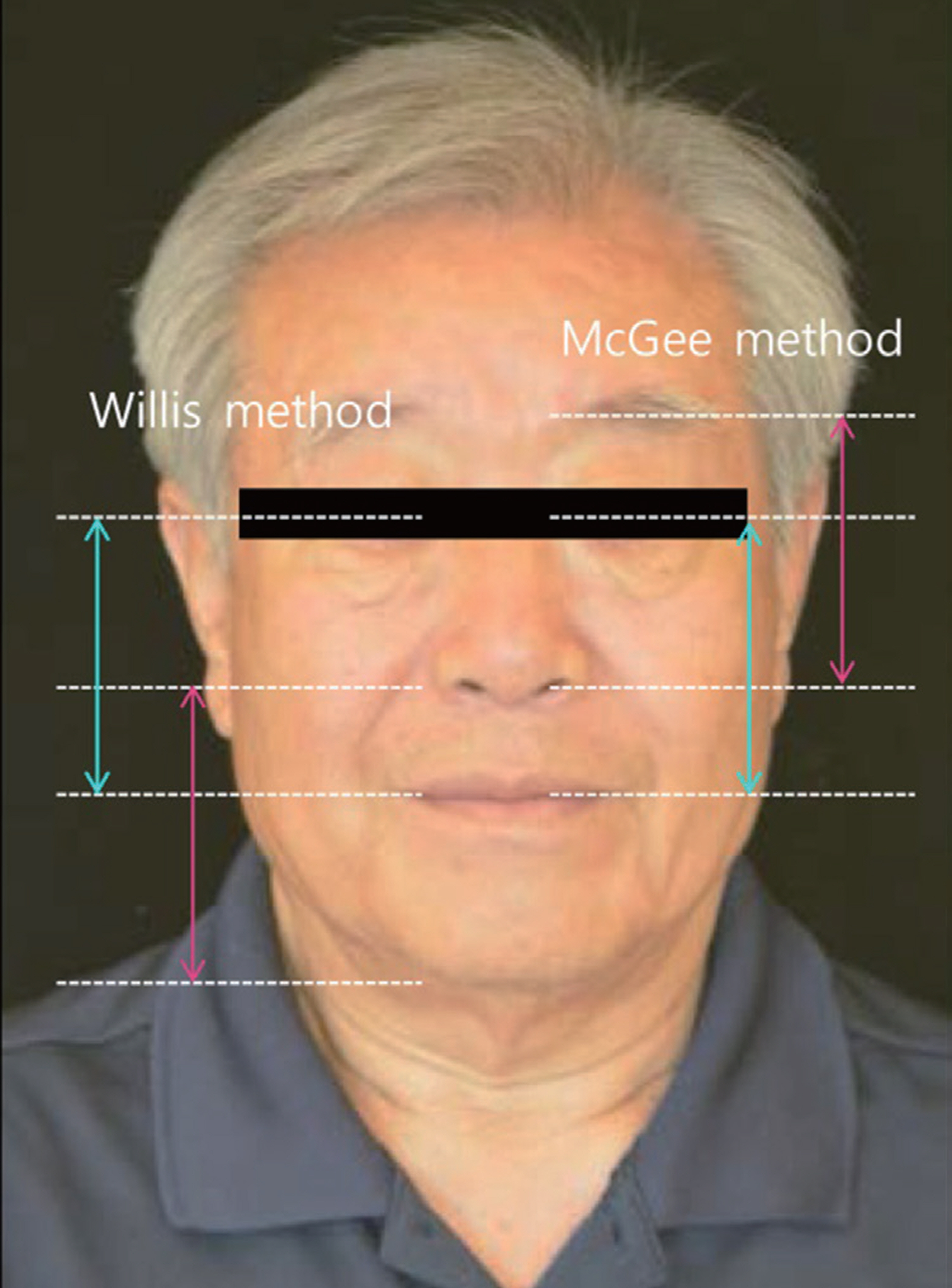
Fig. 7. Evaluation of occlusal vertical dimension using the Willis method and the McGee method.

Fig. 8. (A) Facebow transfer, (B) Mounting procedure to semi-adjustable articulator.

Fig. 9. Reverse curve of Wilson due to excessive occlusal wear.

Fig. 10. Occlusal plane analysis by reference landmarks. (A) Commissure line of lip, (B) Hamular notch-incisive papilla plane, (C) Retromolar pad.

Fig. 11. First provisional restorations. (A) Maxillary occlusal view. Immediate loading after implant installation of maxillary left incisor, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.
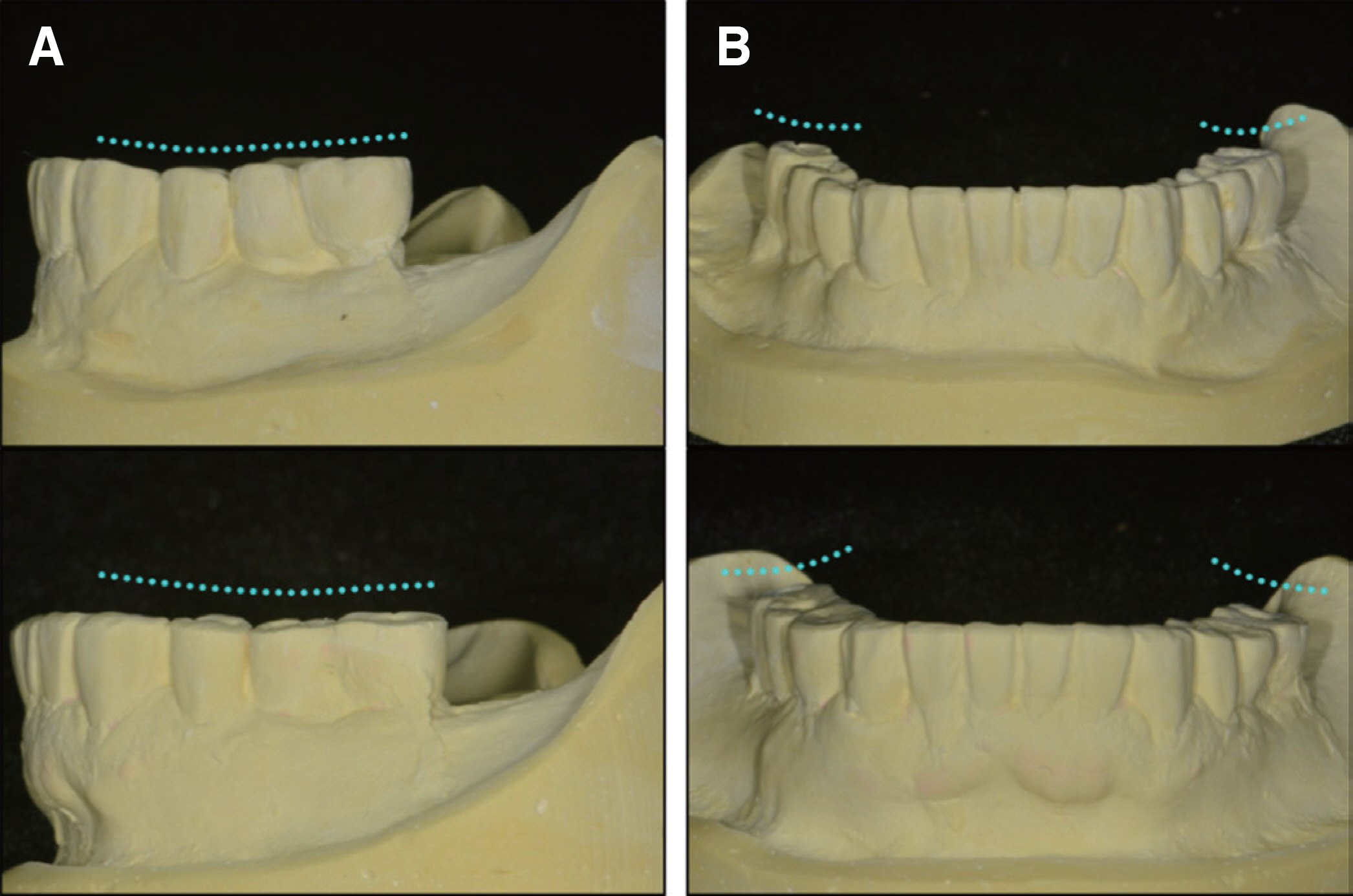
Fig. 12. Occlusal morphology changes of provisional restoration after 2 months. (A) Curve of Spee, (B) Curve of Wilson.

Fig. 13. Adaptive bony changes on the medial wall of the mandibular fossa.

Fig. 14. Axiographic tracing in mastication by ARCUSdigma II. (A) Right TMJ, (B) Hinge axis movement, (C) Left TMJ, (D) Incisor edge in sagittal view, (E) Incisor edge in frontal view, (F) Incisor edge in horizontal view.

Fig. 15. Second provisional restorations with flatter occlusal plane.

Fig. 16. Definitive prosthesis showing harmonious occlusal relationship.

Fig. 17. Periapical radiographs at 1 year follow-up.
Reference
-
1.Calderon PS., Dantas PM., Montenegro SC., Carreiro AF., Oliveira AG., Dantas EM., Gurgel BC. Technical complications with implant-supported dental prostheses. J Oral Sci. 2014. 56:179–84.
Article2.Shanahan TE. The individual occlusal curvature and occlusion. J Prosthet Dent. 1958. 8:230–40.
Article3.Okeson JP. Management of Temporomandibular disorders and occlusion. 7th ed.Mosby; Elsevier Health Sciences;2013.4.The glossary of prosthodontic terms. J Prosthet Dent. 2005. 94:10–92.5.Aull AE. Condylar determinants of occlusal patterns. J Prosthet Dent. 1965. 15:826–49.
Article6.Dawson PE. Functional occlusion: From TMJ to smile design. Mosby;. Elsevier Health Sciences;2006.7.Mongini F. Anatomic and clinical evaluation of the relationship between the temporomandibular joint and occlusion. J Prosthet Dent. 1977. 38:539–51.
Article8.Schuyler CH. The function and importance of incisal guidance in oral rehabilitation. 1963. J Prosthet Dent. 2001. 86:219–32.9.Ow RK., Djeng SK., Ho CK. The relationship of upper facial proportions and the plane of occlusion to anatomic reference planes. J Prosthet Dent. 1989. 61:727–33.10.Oh WS., Alshhrani W., Saglik B., Hansen C. The commissure line of the mouth for orienting the occlusal plane. Int J Prosthodont. 2015. 28:243–5.
Article11.Fu PS., Hung CC., Hong JM., Wang JC. Three-dimensional analysis of the occlusal plane related to the hamular-incisive-papilla occlusal plane in young adults. J Oral Rehabil. 2007. 34:136–40.
Article12.Hall WA Jr. Important factors in adequate denture occlusion. J Prosthet Dent. 1958. 8:764–75.
Article13.Tarnow DP., Emtiaz S., Classi A. Immediate loading of threaded implants at stage 1 surgery in edentulous arches: ten consecutive case reports with 1- to 5-year data. Int J Oral Maxillofac Implants. 1997. 12:319–24.14.Shetty S., Zargar NM., Shenoy K., Rekha V. Occlusal plane location in edentulous patients: a review. J Indian Prosthodont Soc. 2013. 13:142–8.
Article15.Ogawa T., Koyano K., Suetsugu T. Correlation between inclination of occlusal plane and masticatory movement. J Dent. 1998. 26:105–12.
Article16.Ogawa T., Koyano K., Umemoto G. Inclination of the occlusal plane and occlusal guidance as contributing factors in mastication. J Dent. 1998. 26:641–7.
Article17.Karl M., Graef F., Wichmann M., Krafft T. Passivity of fit of CAD/CAM and copy-milled frameworks, veneered frameworks, and anatomically contoured, zirconia ceramic, implant-supported fixed prostheses. J Prosthet Dent. 2012. 107:232–8.
Article18.Cho Y., Raigrodski AJ. The rehabilitation of an edentulous mandible with a CAD/CAM zirconia framework and heat-pressed lithium disilicate ceramic crowns: a clinical report. J Prosthet Dent. 2014. 111:443–7.
Article19.Ehrlich J., Hochman N., Yaffe A. The masticatory pattern as an adjunct for diagnosis and treatment. J Oral Rehabil. 1992. 19:393–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Oral rehabilitation of a patient with collapsed occlusal plane resulting from loss of posterior teeth
- A case of oral rehabilitation in a patient with severe tooth wear and occlusal plane collapse, utilizing maxillary fixed prosthesis and mandibular implant-assisted removable partial denture
- Full mouth rehabilitation of class III patient with disharmonious occlusal plane: A case report
- Full mouth rehabilitation utilizing implant-assisted removable partial denture with a canted occlusal plane: a case report
- Fixed implant rehabilitation of maxillary edentulous patient using intraoral scanning digital workflow: a case report
