Free Vascularized Fibular Graft for Femoral Head Collapse Combined with Ununited Pathologic Intertrochanteric Fracture
- Affiliations
-
- 1Department of Orthopaedic Surgery, Good Samsun Hospital, Busan, Korea. hljo88@hanmail.net
- 2Department of Orthopaedic Surgery, The Catholic University of Korea, Bucheon St. Mary's Hospital, Bucheon, Korea.
- KMID: 2410066
- DOI: http://doi.org/10.4055/jkoa.2018.53.2.174
Abstract
- Surgery for pathologic hip fracture poses significant challenges regarding the fixation of fracture and management of the original tumor lesion. An extensive destruction of the femoral neck and intertrochanteric region by benign or malignant lesions complicated by a pathological fracture generally necessitates total hip arthroplasty; however, in adolescents and young adults, preservation of the hip is preferable. We present a 14-year-old female patient, who sustained a pathological intertrochanteric fracture through a pre-existing aneurysmal bone cyst. Several operative interventions with internal fixation and bone graft were unsuccessful, and combined nonunion and progression of osteolysis around the compression hip screw eventually caused femoral head collapse, mimicking osteonecrosis. Hip preservation and resolution of the original tumor were achieved by free vascularized fibular graft.
MeSH Terms
Figure
-
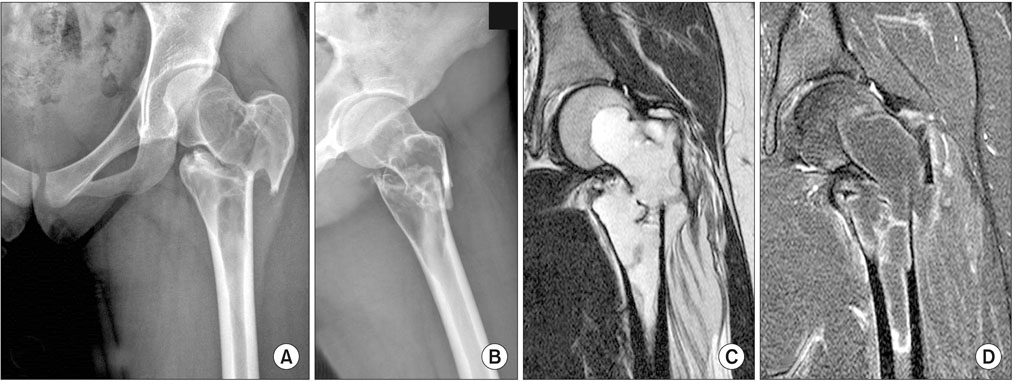
Figure 1 Preoperative anteroposterior (A) and lateral (B) radiographs show a large, multiseptated osteolytic lesion centered around the proximal femur with a displaced intertrochanteric fracture. T2-weighted coronal magnetic resonance image shows a well-defined high signal lesion and subtle fluid-fluid levels within the expansile mass (C) and peripheral enhancing rim with gadolinium (D).
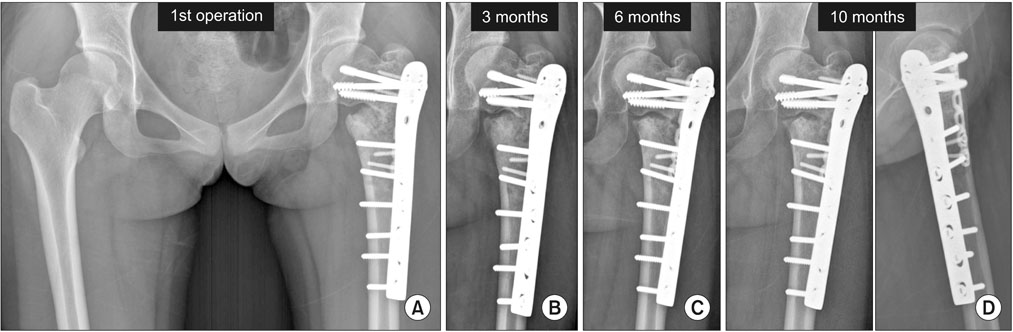
Figure 2 (A) Anteroposterior radiographs after the first operation. Three months (B), six months (C), and 10 months (D) follow-up anteroposterior and lateral radiographs show no progression of union, as well as varus displacement and loosening of the proximal screws.
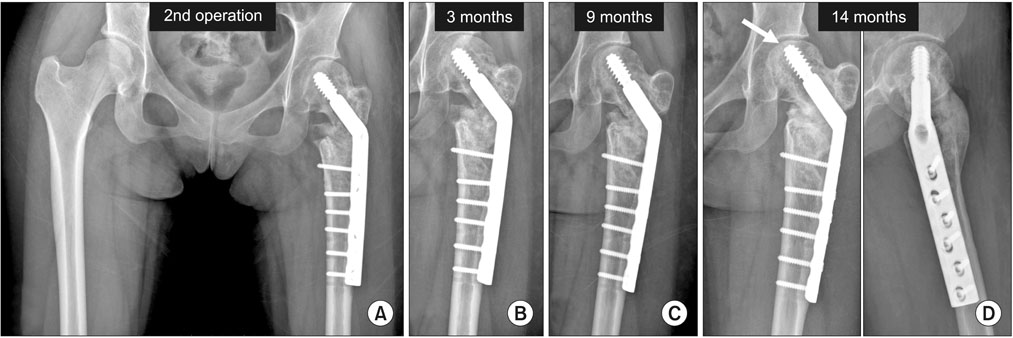
Figure 3 (A) Anteroposterior radiographs after the second operation. Three months (B) and nine months (C) follow-up radiographs show progressive osteolysis around the lag screw in the femoral head. (D) Fourteen months follow-up radiographs show an extensive osteolysis, and subtle femoral head collapse and suspicious subchondral fracture (arrow).
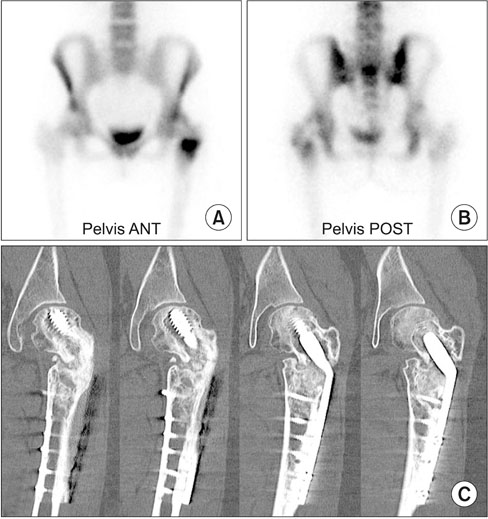
Figure 4 Anterior (ANT; A) and posterior (POST; B) view of technetium-99m bone scintigraphs show a cold area caused by metallic implant and intense uptake in the fracture site, but no significant uptake in the femoral head. (C) Consecutive computed tomographs show a partial union of the anterior portion of intertrochanteric fracture, but clearly show an osteolysis around the lag screw, and subchondral fracture with subsequent collapse of the femoral head.

Figure 5 (A) Immediate postoperative anteroposterior radiograph after the vascularized fibular graft. Six months (B) and one-year (C) follow-up radiographs show progressive union of fracture. (D) Anteroposterior and lateral radiographs five years after the third operation show a complete union of intertrochanteric fracture, a well-incorporated graft, and recovered femoral head collapse.
Reference
-
1. Wai EK, Davis AM, Griffin A, Bell RS, Wunder JS. Pathologic fractures of the proximal femur secondary to benign bone tumors. Clin Orthop Relat Res. 2001; 393:279–286.
Article2. Urbaniak JR, Coogan PG, Gunneson EB, Nunley JA. Treatment of osteonecrosis of the femoral head with free vascularized fibular grafting. A long-term follow-up study of one hundred and three hips. J Bone Joint Surg Am. 1995; 77:681–694.
Article3. Adler CP. Solid aneurysmal bone cyst with pathologic bone fracture. Skeletal Radiol. 1995; 24:214–216.
Article4. Enneking WF, Gearen PF. Fibrous dysplasia of the femoral neck. Treatment by cortical bone-grafting. J Bone Joint Surg Am. 1986; 68:1415–1422.
Article5. Jaffe KA, Dunham WK. Treatment of benign lesions of the femoral head and neck. Clin Orthop Relat Res. 1990; 257:134–137.
Article6. Reddy KI, Sinnaeve F, Gaston CL, Grimer RJ, Carter SR. Aneurysmal bone cysts: do simple treatments work? Clin Orthop Relat Res. 2014; 472:1901–1910.
Article7. Mankin HJ, Hornicek FJ, Ortiz-Cruz E, Villafuerte J, Gebhardt MC. Aneurysmal bone cyst: a review of 150 patients. J Clin Oncol. 2005; 23:6756–6762.
Article8. Beris AE, Lykissas MG, Payatakes A, Kontogeorgakos VA, Mavrodontidis A, Korompilias AV. Free vascularized fibular graft for treatment of pathological femoral neck fracture and osteonecrosis of the femoral head: a case report with a long-term follow-up. Microsurgery. 2009; 29:240–243.
Article9. Lee YK, Yoo JJ, Koo KH, Yoon KS, Min BW, Kim HJ. Collapsed subchondral fatigue fracture of the femoral head. Orthop Clin North Am. 2009; 40:259–265.
Article10. Lenich A, Bachmeier S, Prantl L, et al. Is the rotation of the femoral head a potential initiation for cutting out? A theoretical and experimental approach. BMC Musculoskelet Disord. 2011; 12:79.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Study on the fibular Strut Graft in the Ldiopathic Osteonercrosis of Femoral Head
- Treatment of Large Bone Defect of Femorl Shaft with Vascularized Fibular Graft and Ender Nail: A Case Report
- Vascularized Fibula Graft for Restoration of the Large Bone Defect
- Congenital Pseudarthrosisof the Tibia: Treated with Free Vascularized Fibular Graft
- Free Vascularized Fibular Graft for the Treatment of the Large Bone Defect
