Successful Transjugular Intrahepatic Portosystemic Shunt with Embolization Subsequent to Endoscopic Variceal Band Ligation for Bleeding Anorectal Varices
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Chonnam National University Hospital, Gwangju, Korea. choisk@jnu.ac.kr
- 2Department of Radiology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2409893
- DOI: http://doi.org/10.4166/kjg.2018.71.4.234
Abstract
- Anorectal variceal bleeding is a rare occurrence; however, in such event, it could be fatal due to large size and high blood flow rate of varices. However, to date, there is no standardized treatment modality. Although endoscopic treatment can be provided, in cases of recurrent anorectal variceal bleeding, other therapeutic modalities for hemostasis are necessary. Here, we present a case of 58-year-old female patient with liver cirrhosis, who suffered from massive bleeding of anorectal varices. Endoscopic variceal band ligation was performed for primary hemostasis. Additionally, transjugular intrahepatic portosystemic shunt (TIPS) with embolization was performed to reduce the risk of rebleeding. Following the procedure, she had no further bleeding episodes, and the size of anorectal varices decreased, as seen on an abdomino-pelvic computed tomography. Our case illustrates the effectiveness of combined radiological intervention of TIPS with embolization after endoscopic hemostasis, for variceal obliteration and prevention of rebleeding.
Keyword
MeSH Terms
Figure
-
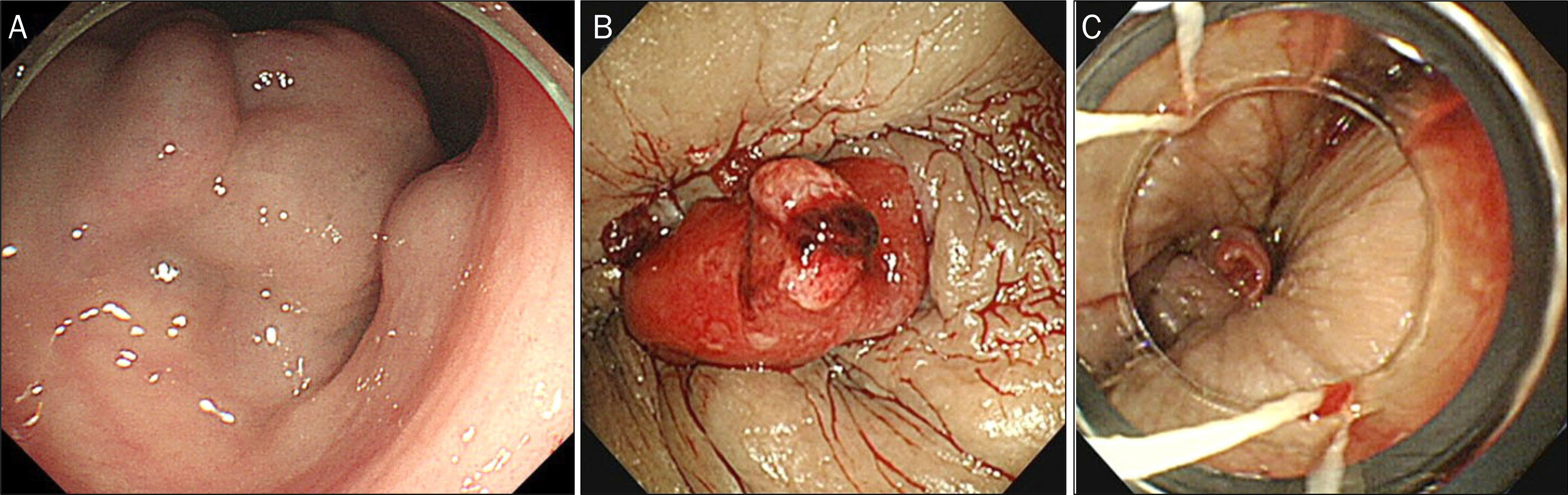
Fig. 1. Sigmoidoscopic finding. Huge anorectal varices (A) and stigmata of recent hemorrhage near the dentate line (B). Endoscopic variceal band ligation was performed to prevent further rebleeding (C).

Fig. 2. An abdominopelvic computed tomography (CT) showing. Huge and tortuous varices in the anorectal region and large amount of ascites in the abdominopelvic cavity (A, B). A follow-up abdominopelvic CT two weeks after TIPS with embolization showed marked improvement of anorectal varices with a decrease in ascites (C, D).

Fig. 3. Portal venogram (contrastenhanced series) obtained after inferior mesenteric vein (IMV) cannulation. Anorectal varices being fed by the tortuous and dilated superior rectal branches arising from the IMV (A). Embolization was performed at both ends of the superior rectal branches using 8 mm Amplatzer vascular plugs (arrowheads) (B).
Reference
-
References
1. Rabinovitz M, Schade RR, Dindzans VJ, Belle SH, Van Thiel DH, Gavaler JS. Colonic disease in cirrhosis. An endoscopic evaluation in 412 patients. Gastroenterology. 1990; 99:195–199.2. Wang TF, Lee FY, Tsai YT, et al. Relationship of portal pressure, anorectal varices and hemorrhoids in cirrhotic patients. J Hepatol. 1992; 15:170–173.
Article3. Maslekar S, Toh EW, Adair R, Bate JP, Botterill I. Systematic review of anorectal varices. Colorectal Dis. 2013; 15:e702–e710.
Article4. Norton ID, Andrews JC, Kamath PS. Management of ectopic varices. Hepatology. 1998; 28:1154–1158.
Article5. Chawla Y, Dilawari JB. Anorectal varices–their frequency in cirrhotic and noncirrhotic portal hypertension. Gut. 1991; 32:309–311.
Article6. Batoon SB, Zoneraich S. Misdiagnosed anorectal varices resulting in a fatal event. Am J Gastroenterol. 1999; 94:3076–3077.
Article7. Takagi S, Kinouchi Y, Takahashi S, Shimosegawa T. Hemodynamics of rectal varices. J Gastroenterol. 2006; 41:611–612.
Article8. Boursier J, Oberti F, Reaud S, Person B, Maurin A, Cales P. Bleeding from rectal varices in a patient with severe decompensated cirrhosis: success of endoscopic band ligation. A case report and review of the literature. Gastroenterol Clin Biol. 2006; 30:783–785.9. Katz JA, Rubin RA, Cope C, Holland G, Brass CA. Recurrent bleeding from anorectal varices: successful treatment with a transjugular intrahepatic portosystemic shunt. Am J Gastroenterol. 1993; 88:1104–1107.10. Ory G, Spahr L, Megevand JM, Becker C, Hadengue A. The long-term efficacy of the intrahepatic portosystemic shunt (TIPS) for the treatment of bleeding anorectal varices in cirrhosis. A case report and review of the literature. Digestion. 2001; 64:261–264.11. Shibata D, Brophy DP, Gordon FD, Anastopoulos HT, Sentovich SM, Bleday R. Transjugular intrahepatic portosystemic shunt for treatment of bleeding ectopic varices with portal hypertension. Dis Colon Rectum. 1999; 42:1581–1585.
Article12. Ahn SS, Kim EH, Kim MD, Lee WJ, Kim SU. Successful hemostasis of intractable rectal variceal bleeding using variceal embolization. World J Gastroenterology. 2015; 21:2558–2562.
Article13. Vangeli M, Patch D, Terreni N, et al. Bleeding ectopic varices–treatment with transjugular intrahepatic portosystemic shunt (TIPS) and embolisation. J Hepatol. 2004; 41:560–566.
Article14. Sakib SM, Kobayashi K, Jawed M. Potential pitfalls in transjugular portosystemic shunt placement for bleeding rectal varices. Case Rep Gastroenterol. 2015; 9:296–301.
Article15. Almadi MA, Almessabi A, Wong P, Ghali PM, Barkun A. Ectopic varices. Gastrointest Endosc. 2011; 74:380–388.
Article16. Helmy A, Al Kahtani K, Al Fadda M. Updates in the pathogenesis, diagnosis and management of ectopic varices. Hepatol Int. 2008; 2:322–334.
Article17. Okada M, Nakashima Y, Kishi T, et al. Percutaneous transhepatic obliteration for massive variceal rectal bleeding. Emerg Radiol. 2012; 19:355–358.
Article18. Kang DH, Park JW, Jeon EY, et al. Successful treatment of bleeding duodenal varix by percutaneous transsplenic embolization. Korean J Gastroenterol. 2015; 66:286–290.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Successful Endoscopic Therapy for Uncontrolled Duodenal Varix after Transjugular Intrahepatic Portosystemic Shunt
- Rescue therapy for bleeding ectopic ileal varices with a transjugular intrahepatic portosystemic shunt and antegrade variceal embolization
- A Case of Successful Treatment of Stomal Variceal Bleeding with Transjugular Intrahepatic Portosystemic Shunt and Coil Embolization
- Transjugular intrahepatic portosystemic shunt and transcatheter embolization treatment of duodenal variceal bleeding
- Gastric Variceal Rebleeding by Aberrant Left Gastric Vein after Transjugular Intrahepatic Portosystemic Shunt: A Case Report
