J Korean Ophthalmol Soc.
2018 Apr;59(4):319-324. 10.3341/jkos.2018.59.4.319.
Treatment Outcome of Wound Infection after Cataract Surgery and Risk Factors of Treatment Failure
- Affiliations
-
- 1Department of Ophthalmology, Chonnam National University Medical School, Gwangju, Korea. kcyoon@jnu.ac.kr
- KMID: 2409679
- DOI: http://doi.org/10.3341/jkos.2018.59.4.319
Abstract
- PURPOSE
To evaluate factors affecting wound infection after cataract surgery, and treatment outcomes.
METHODS
In this retrospective study, we included 20 patients (20 eyes) who experienced wound infection after cataract surgery (phacoemulsification with intraocular lens implantation) between January 2005 and January 2017. Only those who yielded positive microbial smears were selected. All patients were assigned to a "treatment success group" (remission of infection) or a "treatment failure group" (aggravation of infection or a need for surgical intervention to treat an infectious complication). The demographic, clinical and microbiological features of the two groups were compared and binary logistic regression analyses were performed to identify factors affecting treatment failure.
RESULTS
Wound infection developed at 12.25 ± 20.21 days (range 5 to 45 days) after cataract surgery. Sixteen patients developed bacterial and four developed fungal keratitis. Of the 20 patients, 13 (65.0%) were treated successfully and 7 (35.0%) were not. In univariate analyses, diabetes (p = 0.035), incisional suturing (p = 0.038), combined endophthalmitis (p = 0.001), and fungal infection (p = 0.021) were associated with treatment failure. Multivariate analyses showed that combined endophthalmitis (p = 0.001) and fungal infection (p = 0.044) were significant risk factors for treatment failure.
CONCLUSIONS
Cataract wound infection is rare but constitutes a serious complication. Combined endophthalmitis and fungal infection are associated with poor treatment outcomes.
Keyword
MeSH Terms
Figure
-
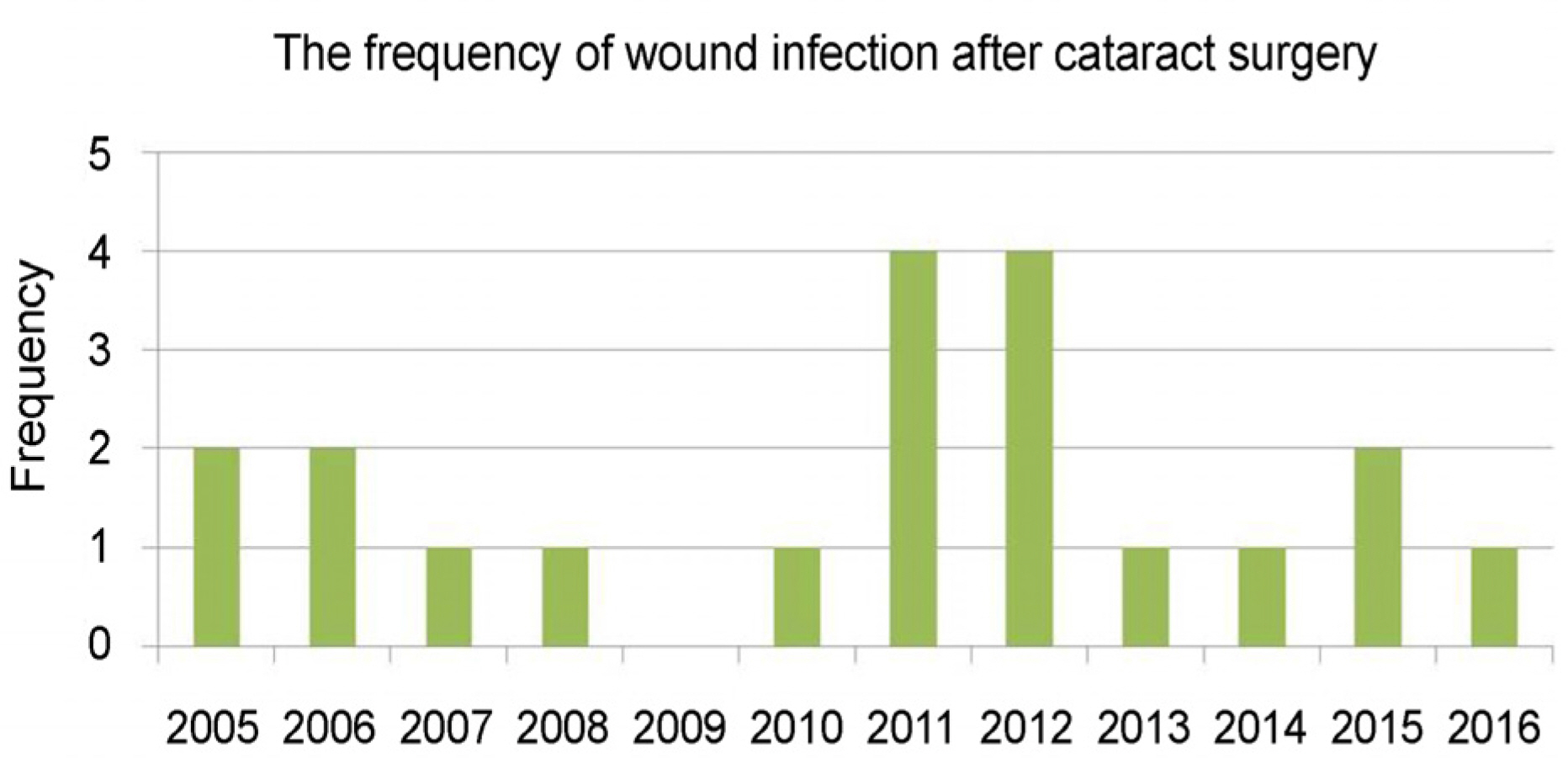
Figure 1. The frequency of wound infection after cataract surgery by year. It shows distribution of occurence in total 20 patients.
Reference
-
1). Aaberg TM Jr, Flynn HW Jr, Schiffman J, et al. Nosocomial acute-onset postoperative endophthalmitis survey. A 10-year review of incidence and outcomes. Ophthalmology. 1998; 105:100410.2). Valenton M. Wound infection after cataract surgery. Jpn J Ophthalmol. 1996; 40:447–55.3). Lopez PF, Beldavs RA, al-Ghamdi S, et al. Pneumococcal endophthalmitis associated with nasolacrimal obstruction. Am J Ophthalmol. 1993; 116:56–62.
Article4). Cosar CB, Cohen EJ, Rapuano CJ, Laibson PR. Clear corneal wound infection after phacoemulsification. Arch Ophthalmol. 2001; 119:1755–9.
Article5). Maxwell DP Jr, Diamond JG, May DR. Surgical wound defects associated with endophthalmitis. Ophthalmic Surg. 1994; 25:157–61.
Article6). Chiang RK, Rapuano CJ. Recurrent methicillin-resistant Staphylococcus aureus wound ulcer after clear-cornea cataract surgery. CLAO J. 2002; 28:109–10.7). Yamamoto N, Matsumoto T, Ishibashi Y. Fungal keratitis caused by Colletotrichum gloeosporioides. Cornea. 2001; 20:902–3.
Article8). McDonnell PJ, Werblin TP, Sigler L, Green WR. Mycotic keratitis due to Beauveria alba. Cornea. 1984-1985; 3:213–6.
Article9). Kau HC, Tsai CC, Kao SC, Liu JH. Corneal ulcer of the side port after phacoemulsification induced by Acinetobacter baumannii. J Cataract Refract Surg. 2002; 28:895–7.
Article10). Rao SK, Madhavan HN, Sitalakshmi G, Padmanabhan P. Norcardia asteroids keratitis: report of seven patients and literature review. Indian J Ophthalmol. 2000; 48:217–21.11). Driebe WT Jr, Mandelbaum S, Forster RK, et al. Pseudophakic endophthalmitis. Diagnosis and management. Ophthalmology. 1986; 93:442–8.12). Scott IU, Flynn HW Jr, Feuer W. Endophthalmitis after secondary intraocular lens implantation. A case-control study. Ophthalmology. 1995; 102:1925–31.13). Kattan HM, Flynn HW Jr, Pflugfelder SC, et al. Nosocomial endophthalmitis survey. Current incidence of infection after intraocular surgery. Ophthalmology. 1991; 98:227–38.14). Menikoff JA, Speaker MG, Marmor M, Raskin EM. A case-control study of risk factors for postoperative endophthalmitis. Ophthalmology. 1991; 98:1761–8.
Article15). Speaker MG, Milch FA, Shah MK, et al. Role of external bacterial flora in the pathogenesis of acute postoperative endophthalmitis. Ophthalmology. 1991; 98:639–49. discussion 650.
Article16). Mendicute J, Orbeqozo J, Ruiz M, et al. Keratomycosis after cataract surgery. J Cataract Refract Surg. 2000; 26:1660–6.
Article17). Garg P, Mahesh S, Bansal AK, et al. Fungal infection of sutureless self-sealing incision for cataract surgery. Ophthalmology. 2003; 110:2173–7.
Article18). Lalitha P, Prajna NV, Kabra A, et al. Risk factors for treatment outcome in fungal keratitis. Ophthalmology. 2006; 113:526–30.
Article19). Nagaki Y, Hayasaka S, Kadoi C, et al. Bacterial endophthalmitis after small-incision cataract surgery, effect of incision placement and intraocular lens type. J Cataract Refract Surg. 2003; 29:20–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk Factors for Glaucoma Filtering Surgery and Mitomycin C
- Factors Affecting Treatment Outcome of Graft Infection Following Penetrating Keratoplasty
- An Obseration on Operations upon Diabetic Cataracts
- Postoperative Spine Infections
- Incidence and Risk Factors for Implant Failure in Spinal Metastasis Surgery
