Rapidly Growing Anaplastic Ganglioglioma Mimicking Brain Metastasis in a Middle-Aged Woman: A Case Report
- Affiliations
-
- 1Department of Radiology, Inha University Hospital, Incheon, Korea. pengoon@gmail.com
- 2Department of Pathology, Inha University Hospital, Incheon, Korea.
- 3Department of Neurosurgery, Inha University Hospital, Incheon, Korea.
- KMID: 2408264
- DOI: http://doi.org/10.3348/jksr.2018.78.2.135
Abstract
- Anaplastic gangliogliomas (AGGs), the malignant counterpart of gangliogliomas, are classified as grade III tumors by the World Health Organization. Although, the clinical course and optimal treatment of AGGs are not well understood, they often result in worse local control rate and shorter survival. The authors describe the magnetic resonance imaging findings of a middle-aged woman with supratentorial AGG, that manifested as a rapidly growing cystic mass which mimicked metastasis. The authors suggest that AGG may be considered as a possible diagnosis for a rapidly growing peripheral enhancing mass in the brain, especially when it is superficially located.
MeSH Terms
Figure
-
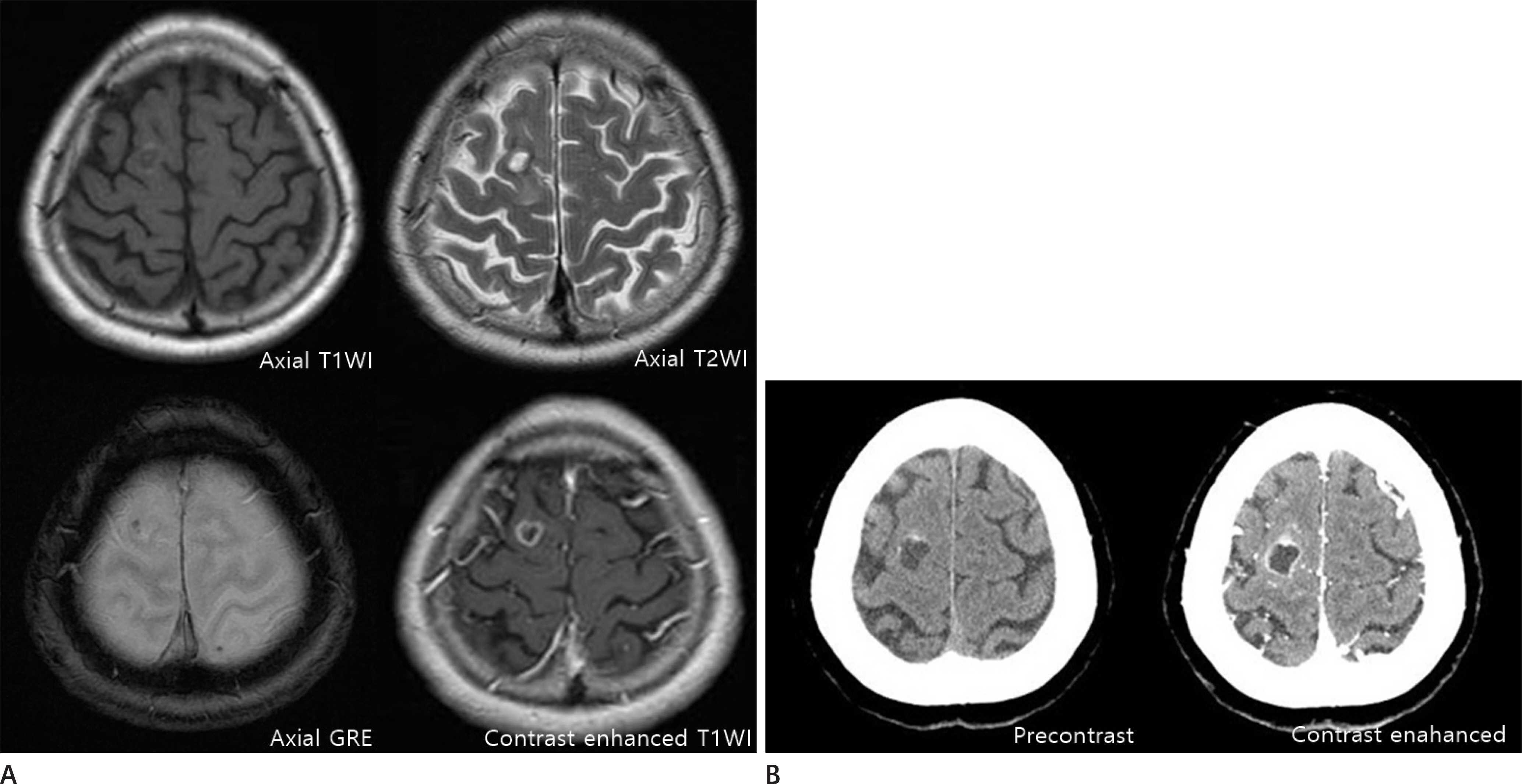
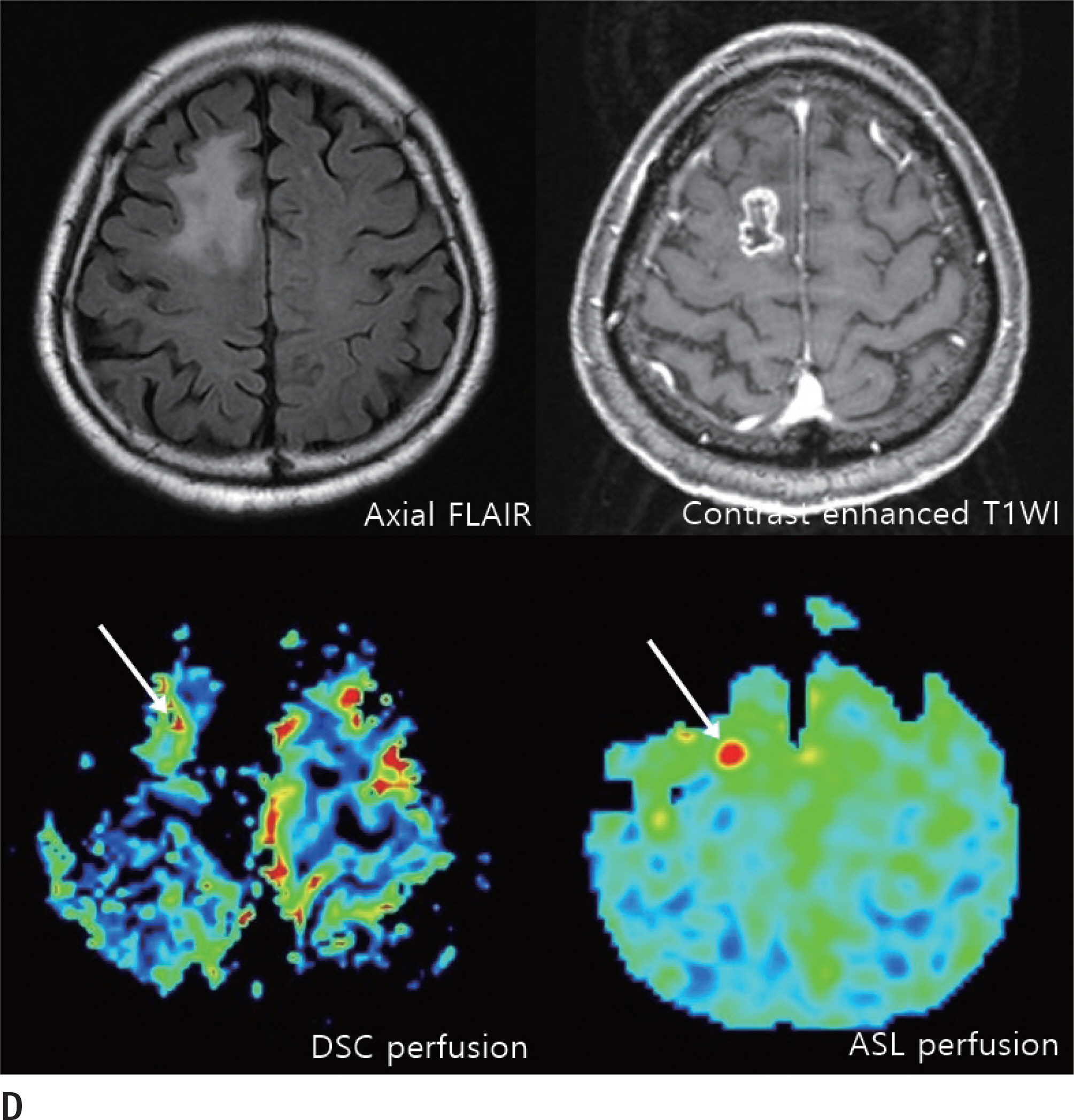
Fig. 1. Anaplastic ganglioglioma with rapid tumor growth in a 68-year-old woman. A. Axial T1 (left upper panel) and T2 (right upper panel) magnetic resonance images showing a cystic mass with a mild surrounding edema in the right superior frontal gyrus. The gradient echo image (left under panel) shows a dark signal intensity within the mass, suggesting calcification or hemorrhage. The contrast-enhanced T1WI (right under panel) shows a peripheral ring enhancement. B. Approximately 2 months after the initial magnetic resonance scan, follow-up precontrast- (left panel) and contrast-enhanced (right panel) brain computed tomography images showing a rapidly growing peripheral enhancing cystic mass with septation and peripheral calcification in the right superior frontal gyrus, with a maximum diameter of 1.6 cm. GRE = gradient echo sequence, T1WI = T1-weighted image, T2WI = T2-weighted image Anaplastic ganglioglioma with rapid tumor growth in a 68-year-old woman. C. Microscopic finding showing the histopathological features of anaplastic ganglioglioma in our case. Biphasic neoplasm with calcification. Neuronal (black arrowhead) and astrocytic components (white arrowhead; H&E, original magnification, × 40, left upper panel). The immunostaining features are suggestive of ganglioglioma. The neoplastic glial components are positive for Olig2 (anti-Olig2 immunohistochemistry, × 40, right upper panel), and the ganglion cells are positive for NeuN (anti-NeuN immunohistochemistry, × 40, left under panel). Anaplastic pathological features include focal necrosis and endothelial proliferation (H&E, original magnification, × 100, right under panel). H&E = hematoxylin-eosin stain Anaplastic ganglioglioma with rapid tumor growth in a 68-year-old woman. D. Postoperative evaluation was performed 3 months after the surgical resection. FLAIR (left upper panel) and contrast-enhanced (right upper panel) magnetic resonance images showing an irregular peripheral enhancing lesion with a maximum diameter of 1.9 cm and a surrounding edema along the resection margin. DSC perfusion image (left under panel) shows increased cerebral blood volume (white arrow), and ASL perfusion image (right under panel) shows increased cerebral blood flow (white arrow). These findings suggest tumor recurrence. ASL = arterial spin labelling, DSC = dynamic susceptibility contrast, FLAIR = fluid-attenuated inversion recovery, T1WI = T1-weighted image

Reference
-
References
1. Zentner J, Wolf HK, Ostertun B, Hufnagel A, Campos MG, Solymosi L, et al. Gangliogliomas: clinical, radiological, and histopathological findings in 51 patients. J Neurol Neurosurg Psychiatry. 1994; 57:1497–1502.
Article2. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007; 114:97–109.
Article3. Luyken C, Blümcke I, Fimmers R, Urbach H, Wiestler OD, Schramm J. Supratentorial gangliogliomas: histopathologic grading and tumor recurrence in 184 patients with a median follow-up of 8 years. Cancer. 2004; 101:146–155.
Article4. Zanello M, Pages M, Tauziède-Espariat A, Saffroy R, Puget S, Lacroix L, et al. Clinical, imaging, histopathological and molecular characterization of anaplastic ganglioglioma. J Neuropathol Exp Neurol. 2016; 75:971–980.
Article5. Hirose T, Kannuki S, Nishida K, Matsumoto K, Sano T, Hiza-wa K. Anaplastic ganglioglioma of the brain stem demonstrating active neurosecretory features of neoplastic neuronal cells. Acta Neuropathol. 1992; 83:365–370.
Article6. Fink KR, Fink JR. Imaging of brain metastases. Surg Neurol Int. 2013; 4(Suppl 4):S209–S219.
Article7. Toh CH, Castillo M, Wong AM, Wei KC, Wong HF, Ng SH, et al. Primary cerebral lymphoma and glioblastoma multi-forme: differences in diffusion characteristics evaluated with diffusion tensor imaging. AJNR Am J Neuroradiol. 2008; 29:471–475.
Article8. Choudry UK, Khan SA, Qureshi A, Bari E. Primary anaplastic pleomorphic xanthoastrocytoma in adults. Case report and review of literature. Int J Surg Case Rep. 2016; 27:183–188.
Article9. Lang FF, Epstein FJ, Ransohoff J, Allen JC, Wisoff J, Abbott IR, et al. Central nervous system gangliogliomas. J Neurosurg. 1993; 79:867–873.
Article10. Selvanathan SK, Hammouche S, Salminen HJ, Jenkinson MD. Outcome and prognostic features in anaplastic ganglioglioma: analysis of cases from the SEER database. J Neurooncol. 2011; 105:539–545.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anaplastic Ganglioglioma in a Middle-aged Woman: A Case Report with a Review of the Literature
- Undiagnosed Anaplastic Ganglioglioma Resulting in the Sudden Unexpected Death of a Young Woman
- Ganglioglioma of the Brain Stem: Case Report
- A Case of Anaplastic Carcinoma of the Pancreas Mimicking a Gastrointestinal Stromal Tumor
- Sudden Death Due to a Ganglioglioma
