Sacral Insufficiency Fractures: How to Classify?
- Affiliations
-
- 1Hannover Region Public Health Department, Hannover Region, Hannover, Germany. gesabakker@gmx.de
- 2Department for Radiology and Neuroradiology, KRH Nordstadt, Hannover, Germany.
- 3Institute for Medical Statistics, Computer Science and Epidemiology IMSIE, University of Cologne, Cologne, Germany.
- 4Department of Traumatology and Orthopedics, KRH Nordstadt, Hannover, Germany.
- KMID: 2408028
- DOI: http://doi.org/10.3340/jkns.2017.0188
Abstract
OBJECTIVE
The diagnosis of insufficiency fractures of the sacrum in an elder population increases annually. Fractures show very different morphology. We aimed to classify sacral insufficiency fractures according to the position of cortical break and possible need for intervention.
METHODS
Between January 1, 2008 and December 31, 2014, all patients with a proven fracture of the sacrum following a low-energy or an even unnoticed trauma were prospectively registered : 117 females and 13 males. All patients had a computer tomography of the pelvic ring, two patients had a magnetic resonance imaging additionally : localization and involvement of the fracture lines into the sacroiliac joint, neural foramina or the spinal canal were identified.
RESULTS
Patients were aged between 46 and 98 years (mean, 79.8 years). Seventy-seven patients had an unilateral fracture of the sacral ala, 41 bilateral ala fractures and 12 patients showed a fracture of the sacral corpus : a total of 171 fractures were analyzed. The first group A included fractures of the sacral ala which were assessed to have no or less mechanical importance (n=53) : fractures with no cortical disruption ("bone bruise") (A1; n=2), cortical deformation of the anterior cortical bone (A2; n=4), and fracture of the anterolateral rim of ala (A3; n=47). Complete fractures of the sacral ala (B; n=106) : parallel to the sacroiliac joint (B1; n=63), into the sacroiliac joint (B2; n=19), and involvement of the sacral foramina respectively the spinal canal (B3; n=24). Central fractures involving the sacral corpus (C; n=12) : fracture limited to the corpus or finishing into one ala (C1; n=3), unidirectional including the neural foramina or the spinal canal or both (C2; n=2), and horizontal fractures of the corpus with bilateral sagittal completion (C3; n=8). Sixty-eight fractures proceeded into the sacroiliac joint, 34 fractures showed an injury of foramina or canal.
CONCLUSION
The new classification allowes the differentiation of fractures of less mechanical importance and a risk assessment for possible polymethyl methacrylate leaks during sacroplasty in the direction of the neurological structures. In addition, identification of instable fractures in need for laminectomy and surgical stabilization is possible.
Keyword
MeSH Terms
Figure
-

Fig. 1 A : Type A-fractures of the sacral ala : A1 with bone bruise (MRI) without a visible fracture line in the CT-scan; A2 deformation of the anterior cortical bone without a cortical disruption; and A3 anterolateral rim fracture of the ala with up to 1 cm distance in the direction of the medial sacroiliac joint. B : A1 with bone bruise in MRI; A2 plasticity of the cortical bone; A3 anterolateral fracture of the ala with up to 1 cm distance in the direction of the medial sacroiliac joint (rim fracture). A1 arrow shows bone bruise; A2 arrow shows plastic deformation of the anterior cortex; A3 arrow shows compression fracture of the anteolateral rim of ala.

Fig. 2 A : Type B fractures of the sacral ala : B1 fracture parallel to the sacroiliac joint; B2 fracture involving the sacroiliac joint; and B3 fracture with an involvement of the neural foramina or the spinal canal. B : B1 fracture parallel to the sacroiliac joint; B2 fracture involving the sacroiliac joint; B3 fracture with a participation of two neural foramina. B1 arrows show fracture following the sacroiliac joint; B2 arrows show the fracture process in the ala; B3 arrows show the involvement of two neural foramina.
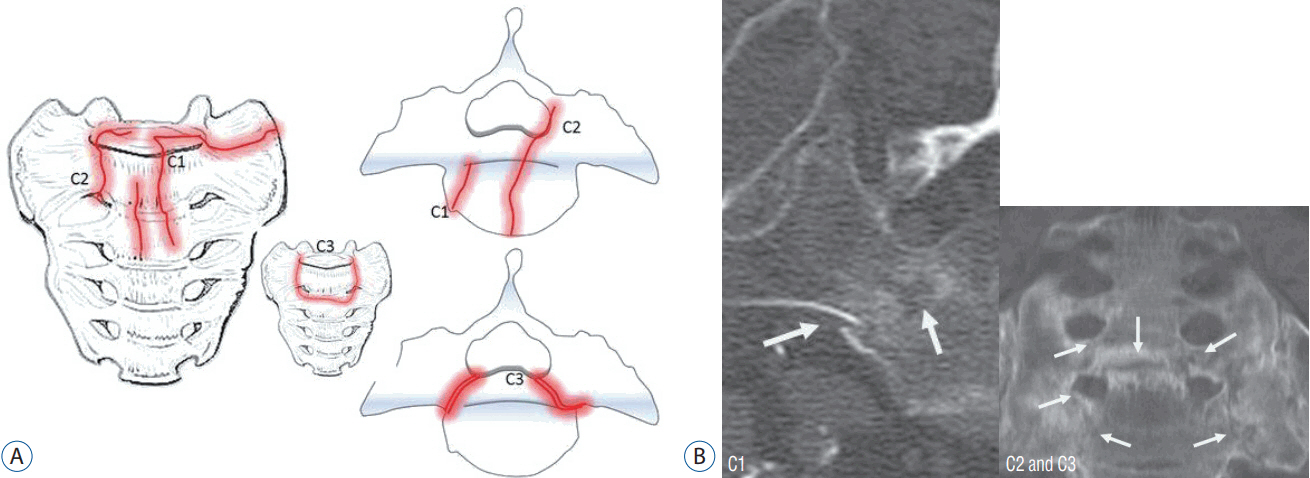
Fig. 3 A : Type C- or corpus-fractures : C1 fracture moves from anterior cortex dorsally or into the sacroiliac joint; C2 fracture with an unilateral involvement of the neural foramina or the spinal canal; and C3 is unstable and represents bilaterally sagittal fractures combined with a transverse leasion. B : C1 fracture of the corpus with an extension in the anterior direction; C2 and C3 bilateral fracture of the corpus with an involvement of the neural foramina which are connected by a transverse fracture. C1 arrows show the fracture development from anterior to the dorsal cortex; C2 and C3 arrows show the bilateral fracture of the corpus, the arrow in the middle shows the fracture connection by a transverse component.
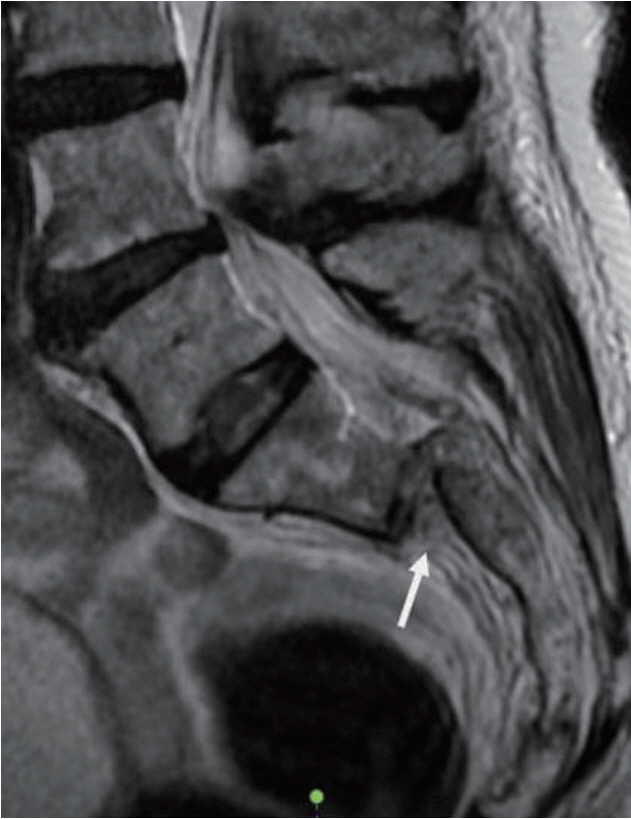
Fig. 4 Sagittal dislocation of type C3 fracture in magnetic resonance imaging. Arrow shows the horizontal dislocation by the transverse corpus fracture.

Fig. 5 Patient number in the distribution of age groups containing 117 females (average age, 79.8 years) and 13 males (average age, 76.9 years); average age of all of 79.5 years (range, 46 to 98 years).
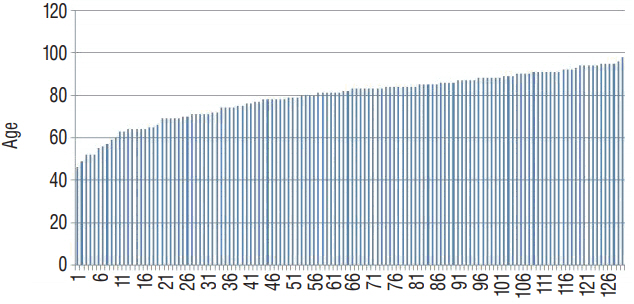
Fig. 6 Age range of 117 females (average age, 79.8 years) and 13 males (average age, 76.9 years) an average of all of 79.5 years (range, 46 to 99).

Fig. 7 Patient number and distribution of unilateral (unilat.) and bilateral (bilat.) ala fractures (types A and B) as well as of corpus fractures (type C).
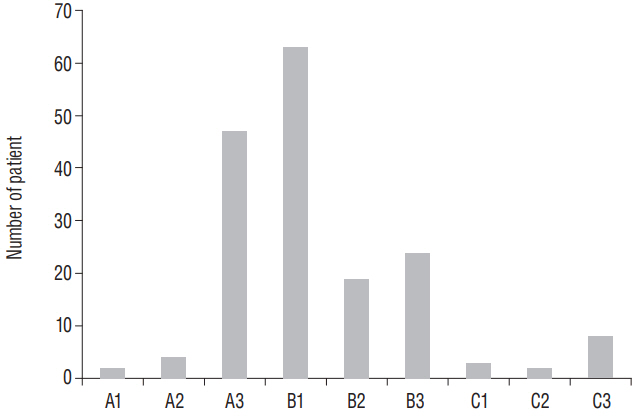
Fig. 8 The most frequent fracture was the fracture of the ala parallel to the sacroiliac joint (type B1) followed by the anterolateral ala rim fracture (type A3). There was an involvement of the spinal canal or the neural foramina in 34 cases (B3, C2, and C3). A corpus fracture was seen in 12 cases, thereof eight patients with a combination of transverse and bilateral sagittal fractures (type C3).
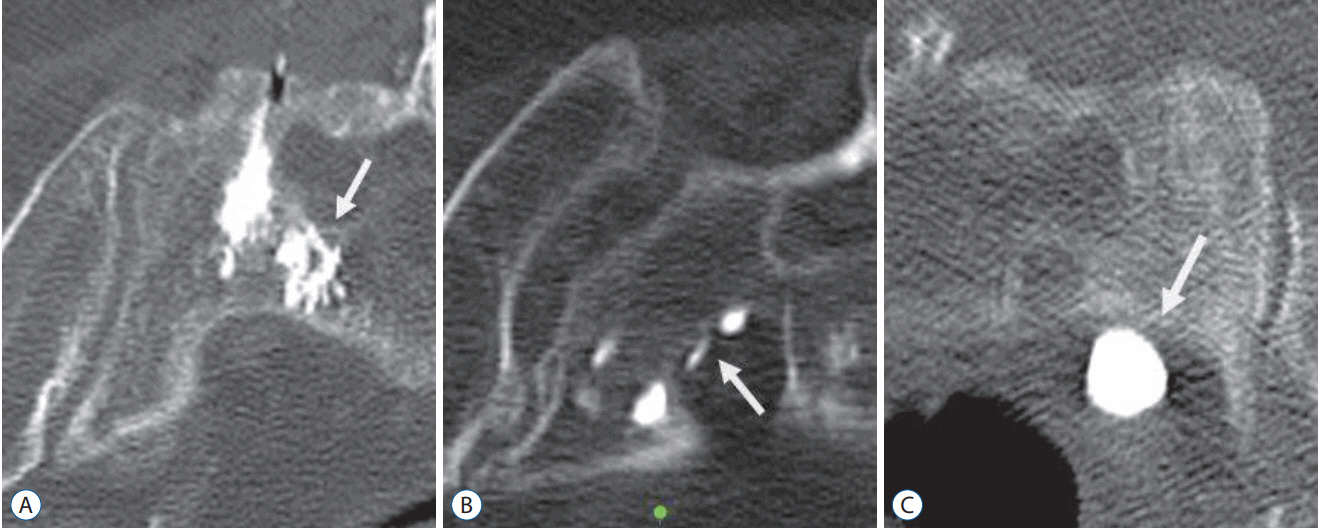
Fig. 9 A : Insertion of PMMA-cement near neurological structures does normally not cause a leakage through the cortical bone. B : In rare cases an uninjured dura seems to stop the leakage. Temporary neurological sensations had been reported. C : If fractures reached the ventral border, a ventral passover was possible. Arrow in (A) shows PMMA-cement position inside the ala. Arrow in (B and C) show PMMA-leakage. PMMA : polymethyl methacrylate.
Reference
-
References
1. Albertsen AM, Egund N, Jurik AG. Fatigue fracture of the sacral bone associated with septic arthritis of the symphysis pubis. Skeletal Radiol. 24:605–607. 1995.
Article2. Alnaib M, Waters S, Shanshal Y, Caplan N, Jones S, St Clair Gibson A, et al. Combined pubic rami and sacral osteoporotic fractures: a prospective study. J Orthop Traumatol. 13:97–103. 2012.
Article3. Aretxabala I, Fraiz E, Pérez-Ruiz F, Ríos G, Calabozo M, Alonso-Ruiz A. Sacral insufficiency fractures. High association with pubic rami fractures. Clin Rheumatol. 19:399–401. 2000.
Article4. Bayley E, Srinivas S, Boszczyk BM. Clinical outcomes of sacroplasty in sacral insufficiency fractures: a review of the literature. Eur Spine J. 18:1266–1271. 2009.
Article5. Choi KC, Shin SH, Lee DC, Shim HK, Park CK. Effects of percutaneous sacroplasty on pain and morbility in sacral insufficiency fracture. J Korean Neurosurg Soc. 60:60–66. 2017.
Article6. Connolly LP, Drubach LA, Connolly SA, Treves ST. Young athletes with low back pain: skeletal scintigraphy of conditions other than pars interarticularis stress. Clin Nucl Med. 29:689–693. 2004.
Article7. Cooper KL, Beabout JW, Swee RG. Insufficiency fractures of the sacrum. Radiology. 156:15–20. 1985.
Article8. Denis F, Davis S, Comfort T. Sacral fractures: an important problem. Retrospective analysis of 236 cases. Clin Orthop Relat Res. 227:67–81. 1988.9. Finiels H, Finiels PJ, Jacquot JM, Strubel D. Fractures of the sacrum caused by bone insufficiency. Meta-analysis of 508 cases. Presse Med. 26:1568–1573. 1997.10. Fujii M, Abe K, Hayashi K, Kosuda S, Yano F, Watanabe S, et al. Honda sign and variants in patients suspected of having a sacral insufficiency fracture. Clin Nucl Med. 30:165–169. 2005.
Article11. Gotis-Graham I, McGuigan L, Diamond T, Portek I, Quinn R, Sturgess A, et al. Sacral insufficiency fractures in the elderly. J Bone Joint Surg Br. 76:882–886. 1994.
Article12. Guilbeau JC, Arrivé L, Maruice F, Nahum H. Spontaneous fracture of the sacrum due to “insufficiency”. An overlooked cause of low lumbago in elderly women. J Radiol. 67:741–744. 1986.13. Hak DJ, Baran S, Stahel P. Sacral fractures: current strategies in diagnosis and management. Orthopedics. 32:752–757. 2009.
Article14. Hatgis J, Granville M, Jacobson RE, Berti A. Sacral insufficiency fractures: recognation and treatment in patients with current lumbar vertebral compression fractures. Cureus. 9:e1008. 2017.15. Heo DH, Park CK. Percutaneus sacroplasty for non-neoplastic osteoporotic sacral insufficiency fractures. Pain Physician. 20:89–94. 2017.16. Isler B. Lumbosacral lesions associated with pelvic ring injuries. J Orthop Trauma. 4:1–6. 1990.
Article17. Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. Preliminary report. J Bone Joint Surg Am. 46:1615–1646. 1964.18. Linstrom NJ, Heiserman JE, Kortman KE, Crawford NR, Baek S, Anderson RL, et al. Anatomical and biomechanical analyses of the unique and consistent locations of sacral insuffiency fractures. Spine (Phila Pa 1976). 34:309–315. 2009.
Article19. Longhino V, Bonora C, Sansone V. The management of sacral stress fractures: current concepts. Clin Cases Miner Bone Metab. 8:19–23. 2011.20. Lourie H. Spontaneous osteoporotic fracture of the sacrum. An unrecognized syndrome of the elderly. JAMA. 248:715–717. 1982.
Article21. Majo NM, Helms CA. Sacral stress fractures in long-distance runners. AJR Am J Roentgenol. 174:727–729. 2000.
Article22. Richards AM, Coleman NW, Knight TA, Belkoff SM, Mears SC. Bone density and cortical thickness in normal, osteopenic, and osteoporotic sacra. J Osteoporos. 2010:504078. 2010.
Article23. Rommens PM, Hofmann A. Comprehensive classification of fragility fractures of the pelvic ring: recommendations for surgical treatment. Injury. 44:1733–1744. 2013.
Article24. Rommens PM, Wagner D, Hofmann A. Surgical management of osteoporotic pelvic fractures: a new challenge. Eur J Trauma Emerg Surg. 38:499–509. 2012.
Article25. Rousière M, Kahan A, Job-Deslandre C. Postpartal sacral fracture without osteoporosis. Joint Bone Spine. 68:71–73. 2001.
Article26. Roy-Camille R, Saillant G, Gagna G, Mazel C. Transverse fracture of the upper sacrum. Suicidal jumper’s fracture. Spine (Phila Pa 1976). 10:838–845. 1985.27. Schindler OS, Watura R, Cobby M. Sacral insufficiency fractures. J Orthop Surg (Hong Kong). 15:339–346. 2007.
Article28. Strange-Vognsen HH, Lebech A. An unusual type of fracture in the upper sacrum. J Orthop Trauma. 5:200–203. 1991.
Article29. Tile M. Acute pelvic fractures: I. Causation and classification. J Am Acad Orthop Surg. 4:143–151. 1996.
Article30. Tötterman A, Glott T, Madsen JE, Røise O. Unstable sacral fractures: associated injuries and morbidity at 1 year. Spine (Phila Pa 1976). 31:E628–E635. 2006.31. Weber M, Hasler P, Gerber H. Insufficiency fractures of the sacrum. Twenty cases and review of the literature. Spine (Phila Pa 1976). 18:2507–2512. 1993.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of S1 Radiculopathy in Sacral Insufficiency Fracture without Fracture Line
- MR Findings of Sacral Insufficiency Fractures in Osteoporotic Patients: Two Cases Report
- Sacral Insufficiency Fracture, Usually Overlooked Cause of Lumbosacral Pain
- Sequential Sacral Insufficiency Fracture After Unilateral Pubic Fractures: A Case Report
- Usefulness of Kyphoplasty in Sacral Insufficiency Fracture: A Case Report
