Ann Rehabil Med.
2014 Apr;38(2):277-281.
Neurological Complication After Low-Voltage Electric Injury: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, St. Vincent's Hospital, The Catholic University of Korea College of Medicine, Suwon, Korea. byhong@catholic.ac.kr
- 2Department of Rehabilitation Medicine, Baek Rehabilitation Hospital Care Affiliation, Hwasun, Korea.
Abstract
- Electrical shock can result in neurological complications, involving both peripheral and central nervous systems, which may present immediately or later on. However, delayed neurological complications caused by low-voltage electric shock are rarely reported. Here, a case of a man suffering from weakness and aphasia due to the delayed-onset of the peripheral nerve injury and ischemic stroke following an electrical shock is presented. Possible mechanisms underlying the neurological complications include thermal injury to perineural tissue, overactivity of the sympathetic nervous system, vascular injury, and histological or electrophysiological changes. Moreover, vasospasms caused by low-voltage alternating current may predispose individuals to ischemic stroke. Therefore, clinicians should consider the possibility of neurological complications, even if the onset of the symptoms is delayed, and should perform diagnostic tests, such as electrophysiology or imaging, when patients present with weakness following an electric injury.
Keyword
MeSH Terms
Figure
-
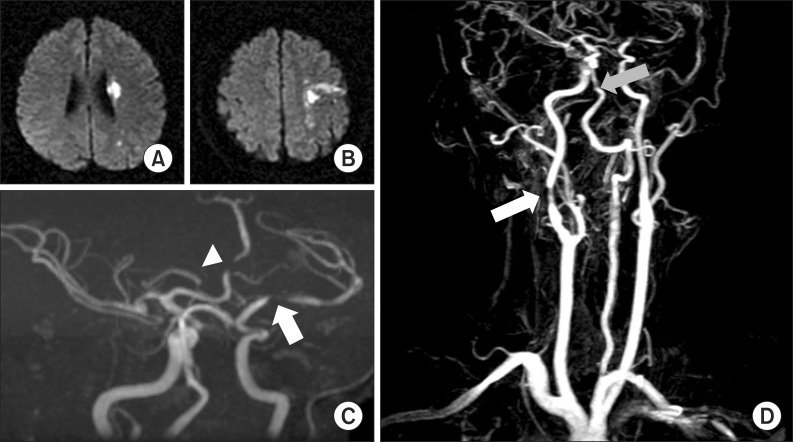
Fig. 1 (A, B) The T2-weighted brain magnetic resonance imaging scan revealed ischemia in left middle cerebral artery territory. (C) Magnetic resonance angiography (MRA) identified marked focal stenosis in the left M1 mid-portion (white arrow) and mid-A2 (white arrowhead). (D) MRA also revealed stenosis of the proximal basilar artery (gray arrow) and the right proximal cervical internal carotid artery (white arrow).
Reference
-
1. Leibovici D, Shemer J, Shapira SC. Electrical injuries: current concepts. Injury. 1995; 26:623–627. PMID: 8550171.
Article2. Cohen JA. Autonomic nervous system disorders and reflex sympathetic dystrophy in lightning and electrical injuries. Semin Neurol. 1995; 15:387–390. PMID: 8848658.
Article3. Kim MW, Kim JH, Lee JM, Paik NJ, Kang MJ, Kim BS. The neuropathy of the electrical burn. J Korean Acad Rehabil Med. 1999; 23:786–791.4. Wilkinson C, Wood M. High voltage electric injury. Am J Surg. 1978; 136:693–696. PMID: 362961.
Article5. Hoover BB, Baxter CR, Kirkpatrick MR. Electromyographic findings in high voltage electrical burns: two cases. South Med J. 1971; 64:1392–1394. PMID: 5126807.
Article6. Solem L, Fischer RP, Strate RG. The natural history of electrical injury. J Trauma. 1977; 17:487–492. PMID: 875082.
Article7. Grube BJ, Heimbach DM, Engrav LH, Copass MK. Neurologic consequences of electrical burns. J Trauma. 1990; 30:254–258. PMID: 2156085.
Article8. Cherington M, Yarnell P, Lammereste D. Lightning strikes: nature of neurological damage in patients evaluated in hospital emergency departments. Ann Emerg Med. 1992; 21:575–578. PMID: 1570918.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transient Quadriplegia after Low-Voltage Electric Shock
- Right Thalamic Hemorrhage Resulting from Low-voltage Electrical Injury: A Case Report
- Delayed Spinal Cord Injury Following Low Voltage Electrical Accident
- Erectile Dysfunction in Patients with Electrical Injury
- Clinical Analysis of Low Voltage Electrical Injury in One Emergency Center
