Multifocal Bilateral Breast Cancer and Breast Follicular Lymphoma: A Simple Coincidence?
- Affiliations
-
- 1First Department of Surgery, Laiko Hospital, University of Athens, Athens, Greece. amichalinos@hotmail.com
- 2Department of Haematology, Laiko Hospital, University of Athens, Athens, Greece.
- 3First Department of Pathology, University of Athens, Athens, Greece.
- KMID: 2407579
- DOI: http://doi.org/10.4048/jbc.2015.18.3.296
Abstract
- Breast cancer coexisting with lymphoma is a rare condition with various diagnostic and therapeutic implications. In this report, we describe the case of a 55-year-old Caucasian woman who presented with simultaneous ductal carcinoma in situ of the right breast, and follicular lymphoma involving an inguinal lymph node and the left breast. The patient underwent local excision and radiotherapy for the ductal carcinoma in situ, while a watch and wait strategy was adopted for the lymphoma. Two years later, the patient presented with multifocal ductal carcinoma of the left breast and reappearance of the lymphoma in the left axillary lymph nodes. She underwent bilateral mastectomy, left sentinel node biopsy, and chemotherapy. Synchronous follicular lymphoma and bilateral metachronous breast carcinoma has not been described previously. Diagnosis is based on tissue histology after excision or a needle biopsy. Treatment for these two diseases is distinct, and a multidisciplinary approach should be adopted.
Keyword
MeSH Terms
Figure
-
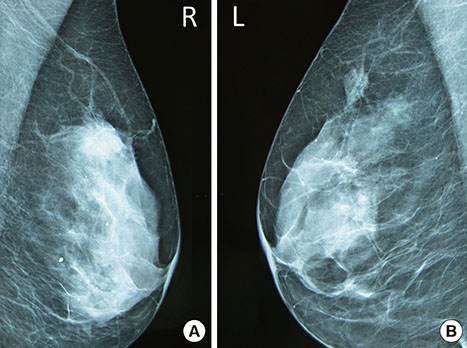
Figure 1 Bilateral mammography of the patient. Both breasts are heterogeneously dense. (A) Right: There is a high-density irregular mass in the upper outer quadrant of the breast. It has indistinct margins, possibly spiculated at places but without significant architectural distortion. The mammogram was graded as Breast Imaging Reporting and Data System (BI-RADS) category 4. (B) Left: There is an asymmetric density with microcalcifications in the upper outer quadrant of the breast corresponding to the palpable lump. The finding has ill-defined or microlobulated margins at places and is not associated with architectural distortion. The mammogram was graded as BI-RADS category 4.
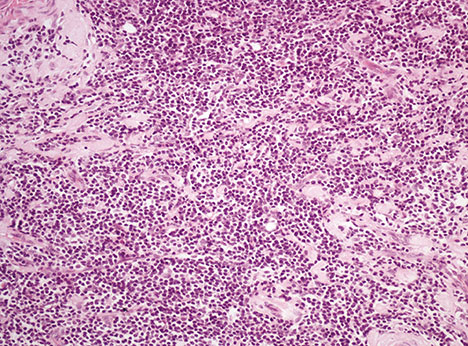
Figure 2 Microscopic finding of secondary follicular lymphoma involving left breast. Neoplastic lymphoid cells, mainly centrocytes with a few scattered centroblasts, diffusely infiltrating breast parenchyma (H&E stain, × 200).
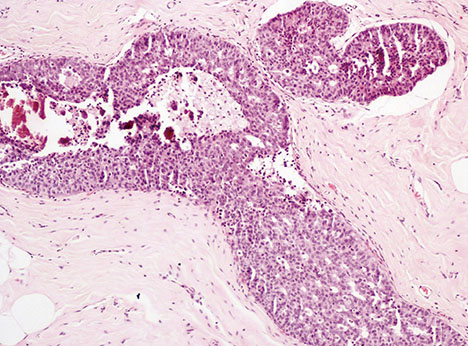
Figure 3 Microscopic findings of right breast ductal carcinoma in situ (DCIS). Low grade DCIS of cribriform pattern with the presence comedo necrosis involving two ducts (H&E stain, ×200).
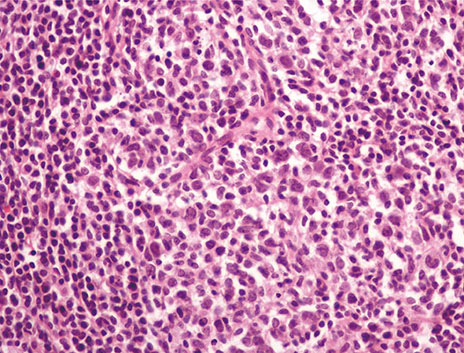
Figure 4 Microscopic findings of inguinal lymph node specimen. Neoplastic lymphoid cells consisting of centrocytes and some few centroblasts (<15/high-power field) infiltrated the inguinal lymph node, thus disturbing the lymph node normal architecture. The neoplastic populating is arranges in a predominantly nodular pattern (H&E stain, ×200).
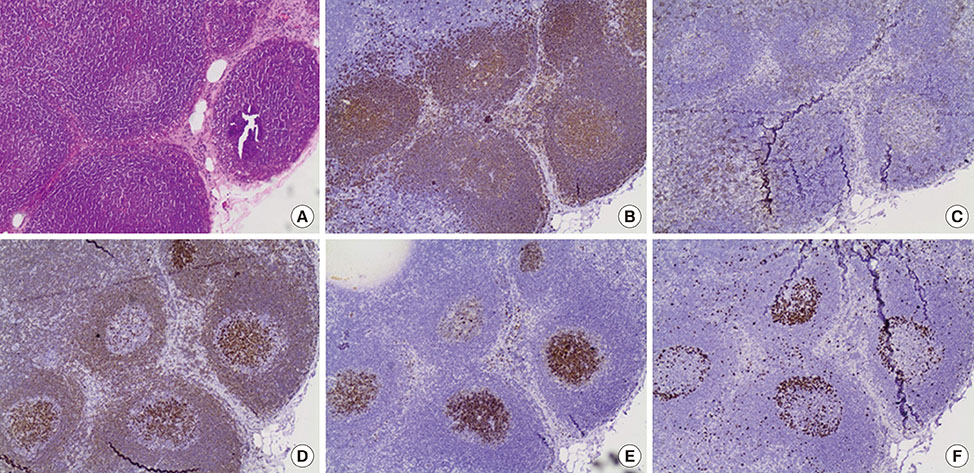
Figure 5 Histological specimen of sentinel lymph node after second excision. (A) Histological examination of in situ follicular lymphoma in sentinel lymph node after second excision (H&E stain, ×100). (B) CD20 immunopositivity showing the nodules corresponding to infiltrated germinal centers (×100). (C) CD3 immunohistochemical staining showing the reactive T cells arranged mainly outside the nodules (×100). (D) Bcl-2 immunopositivity in the lymphoma B cells inside the germinal centers (×100). (E) CD10 immunopositivity in the neoplastic nodules excluding the probability of being primary follicles, the latter being CD10 negative (×100). (F) Ki-67 index in the neoplastic nodules which is rather low, compared to the expected increased one in reactive germinal centers (×100).
Reference
-
1. Laudenschlager MD, Tyler KL, Geis MC, Koch MR, Graham DB. A rare case of synchronous invasive ductal carcinoma of the breast and follicular lymphoma. S D Med. 2010; 63:123–125.2. Cuff KE, Dettrick AJ, Chern B. Synchronous breast cancer and lymphoma: a case series and a review of the literature. J Clin Pathol. 2010; 63:555–557.
Article3. Cox J, Lunt L, Webb L. Synchronous presentation of breast carcinoma and lymphoma in the axillary nodes. Breast. 2006; 15:246–252.
Article4. Barranger E, Marpeau O, Uzan S, Antoine M. Axillary sentinel node involvement by breast cancer coexisting with B-cell follicular lymphoma in nonsentinel nodes. Breast J. 2005; 11:227–228.
Article5. Cohen PL, Brooks JJ. Lymphomas of the breast: a clinicopathologic and immunohistochemical study of primary and secondary cases. Cancer. 1991; 67:1359–1369.
Article6. Cheung KJ, Tam W, Chuang E, Osborne MP. Concurrent invasive ductal carcinoma and chronic lymphocytic leukemia manifesting as a collision tumor in breast. Breast J. 2007; 13:413–417.
Article7. Wiseman C, Liao KT. Primary lymphoma of the breast. Cancer. 1972; 29:1705–1712.
Article8. Tamaoki M, Nio Y, Tsuboi K, Nio M, Tamaoki M, Maruyama R. A rare case of non-invasive ductal carcinoma of the breast coexisting with follicular lymphoma: a case report with a review of the literature. Oncol Lett. 2014; 7:1001–1006.
Article9. Arana S, Vasquez-Del-Aguila J, Espinosa M, Peg V, Rubio IT. Lymphatic mapping could not be impaired in the presence of breast carcinoma and coexisting small lymphocytic lymphoma. Am J Case Rep. 2013; 14:322–325.
Article10. Miles EF, Jacimore LL. Synchronous bilateral breast carcinoma and axillary non-Hodgkin lymphoma: a case report and review of the literature. Case Rep Oncol Med. 2012; 2012:685919.
Article11. Garg NK, Bagul NB, Rubin G, Shah EF. Primary lymphoma of the breast involving both axillae with bilateral breast carcinoma. World J Surg Oncol. 2008; 6:52.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Incidentally detected insitu ductal carcinoma with mastitis
- Concurrent Invasive Ductal Carcinoma of the Breast and Malignant Follicular Lymphoma, Initially Suspected to Be Metastatic Breast Cancer: A Case Report
- Breast Lymphoma: A Report of 2 Cases
- Primary Follicular Lymphoma in a Male Breast: A Case Report
- Bilateral breast carcinoma
