Autotransplantation: A biological treatment alternative for a patient after traumatic dental injury
- Affiliations
-
- 1Division of Orthodontics, School of Dental Medicine, University of Connecticut, Farmington, CT, USA. minnie.vishwanath@unmc.edu
- 2Department of Growth and Development, Orthodontic Section, College of Dentistry, University of Nebraska Medical Center, Lincoln, NE, USA.
- 3Division of Orthodontics, School of Dentistry, University of Louisville, Louisville, KY, USA.
- 4Private Practice, Spring, TX, USA.
- KMID: 2406821
- DOI: http://doi.org/10.4041/kjod.2018.48.2.125
Abstract
- Traumatic dental injury is considered a public dental health problem because of a high childhood incidence, high treatment costs, and prolonged treatment time. Although management guidelines for traumatized teeth have been outlined, tooth loss following trauma is occasionally unavoidable. Here, we describe the successful interdisciplinary management of a traumatized central incisor in an 11-year old boy that was extracted because of a poor prognosis and restored by the autotransplantation of an immature donor tooth into the site. The patient underwent orthodontic treatment in order to close the donor site space and bring the autotransplanted tooth to an ideal position. Postorthodontic treatment radiographs and photographs revealed an esthetic and functional natural tooth replacing the lost tooth. The findings from this case suggest that autotransplantation offers unique advantages as a treatment modality for the restoration of missing teeth, particularly in growing children.
Keyword
MeSH Terms
Figure
-
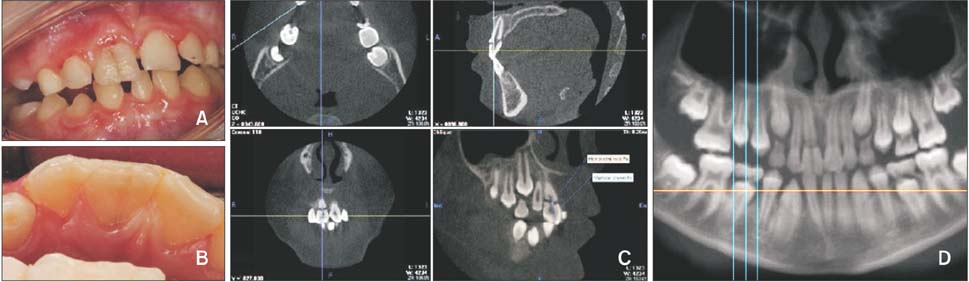
Figure 1 Pretreatment photographs and imaging findings for an 11-year-old boy with a traumatized maxillary central incisor. A, Intraoral photograph shows the crown of the maxillary right central incisor with a vertical fracture line extending onto the labial surface. B, Intraoral photograph shows the crown of the maxillary right central incisor with a vertical fracture line extending onto the palatal surface. C, Cone-beam computed tomography (CBCT) reveals the presence of a horizontal fracture at the cementoenamel junction/coronal portion of the root of the maxillary right central incisor. D, A panoramic radiograph reconstructed from the CBCT data reveals the presence of a vertical crown fracture as well as the root morphology and developmental stage of the mandibular right second premolar.
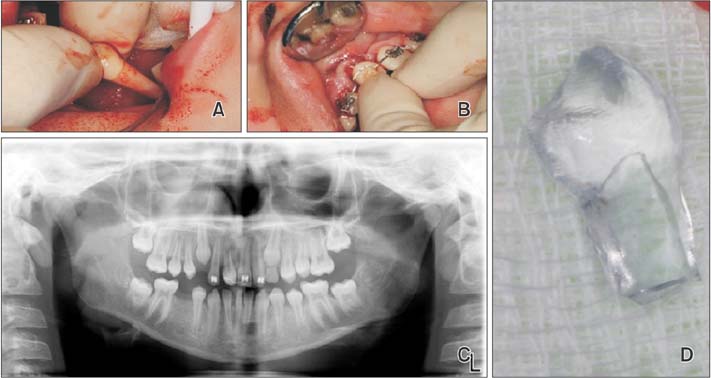
Figure 2 Extraction and autotransplantation of the fractured maxillary central incisor. A, Atraumatic extraction of the mandibular right second premolar (donor tooth). B, Autotransplantation of the mandibular right second premolar into the socket of the maxillary right central incisor. The autotransplanted tooth is splinted to the adjacent incisors using a 0.020-inch stainless steel wire. C, Pretreatment panoramic radiograph shows alveolar bone remodeling around the autotransplanted tooth (tooth #45 in the socket of tooth #11) and the edentulous space of the donor tooth. D, A stereolithographic model of the donor tooth.
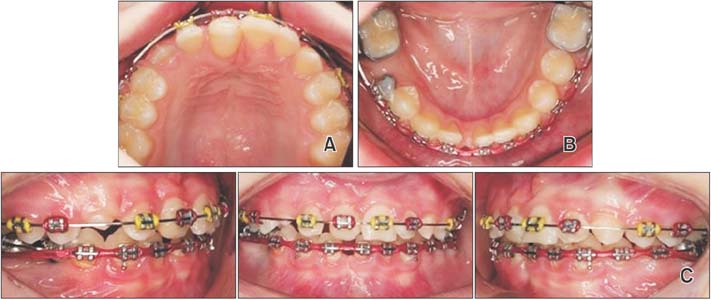
Figure 3 Orthodontic treatment in progress. A, Autotransplanted tooth bonded and aligned with the contralateral central incisor. B, A temporary anchorage device is placed on the ridge for closure of the donor space through protraction of the right mandibular molar. C, Maxillary arch held passively to allow for eruption of maxillary canines bilaterally. Space closure in progress in the mandibular arch.

Figure 4 Intraoral photographs and a panoramic radiograph obtained after autotransplantation and orthodontic treatment. A, Intraoral photographs show functional occlusion and the postrestorative findings for the autotransplanted tooth (tooth #45 in the socket of tooth #11). B, Post-treatment panoramic radiograph showing complete root formation of the autotransplanted tooth.
Reference
-
1. Glendor U. Epidemiology of traumatic dental injuries--a 12 year review of the literature. Dent Traumatol. 2008; 24:603–611.
Article2. Petersson EE, Andersson L, Sörensen S. Traumatic oral vs non-oral injuries. Swed Dent J. 1997; 21:55–68.3. Andreasen JO. The dental trauma guide [Internet]. Copenhagen: Copenhagen University Hospital and the International Association of Dental Traumatology (IADT);2010. cited 2016 Feb 28. Available from: http://dentaltraumaguide.org.4. Cross D, El-Angbawi A, McLaughlin P, Keightley A, Brocklebank L, Whitters J, et al. Developments in autotransplantation of teeth. Surgeon. 2013; 11:49–55.
Article5. Hale ML. Autogenous transplants. J Am Dent Assoc. 1954; 49:193–198.
Article6. Miller HM. Transplantation and reimplantation of teeth. Oral Surg Oral Med Oral Pathol. 1956; 9:84–95.
Article7. Slagsvold O, Bjercke B. Autotransplantation of premolars with partly formed roots. A radiographic study of root growth. Am J Orthod. 1974; 66:355–366.8. Andreasen JO, Kristerson L. Evaluation of different types of autotransplanted connective tissues as potential periodontal ligament substitutes. An experimental replantation study in monkeys. Int J Oral Surg. 1981; 10:189–201.
Article9. Andreasen JO. Periodontal healing after replantation and autotransplantation of incisors in monkeys. Int J Oral Surg. 1981; 10:54–61.
Article10. Andreasen JO, Paulsen HU, Yu Z, Ahlquist R, Bayer T, Schwartz O. A long-term study of 370 autotransplanted premolars Part I Surgical procedures and standardized techniques for monitoring healing. Eur J Orthod. 1990; 12:3–13.
Article11. Park JH, Tai K, Hayashi D. Tooth autotransplantation as a treatment option: a review. J Clin Pediatr Dent. 2010; 35:129–135.
Article12. Tsukiboshi M. Autotransplantation of teeth: requirements for predictable success. Dent Traumatol. 2002; 18:157–180.
Article13. Czochrowska EM, Stenvik A, Album B, Zachrisson BU. Autotransplantation of premolars to replace maxillary incisors: a comparison with natural incisors. Am J Orthod Dentofacial Orthop. 2000; 118:592–600.
Article14. Zaleckiene V, Peciuliene V, Brukiene V, Drukteinis S. Traumatic dental injuries: etiology, prevalence and possible outcomes. Stomatologija. 2014; 16:7–14.15. Chesterman J, Chauhan R, Patel M, Chan MF. The management of traumatic tooth loss with dental implants: part 1. Br Dent J. 2014; 217:627–633.
Article16. Bernard JP, Schatz JP, Christou P, Belser U, Kiliaridis S. Long-term vertical changes of the anterior maxillary teeth adjacent to single implants in young and mature adults. A retrospective study. J Clin Periodontol. 2004; 31:1024–1028.
Article17. Czochrowska EM, Stenvik A, Bjercke B, Zachrisson BU. Outcome of tooth transplantation: survival and success rates 17-41 years posttreatment. Am J Orthod Dentofacial Orthop. 2002; 121:110–119.
Article18. Jung RE, Pjetursson BE, Glauser R, Zembic A, Zwahlen M, Lang NP. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin Oral Implants Res. 2008; 19:119–130.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Autotransplantation combined with orthodontic treatment: a case involving the maxillary central incisors with root resorption after traumatic injury
- Cases report of autotransplantation of immature teeth
- Autotransplantation of the missing tooth: the report of cases
- Evaluation of Autotransplantation
- Splenic Autotransplantation after Blunt Spleen Injury in Children
