Patient-Ventilator Dyssynchrony
- Affiliations
-
- 1Intensive Care Unit, University Hospital of Heraklion, Heraklion, Greece. akoumianakievangelia@gmail.com
- 2Medical School, University of Crete, Heraklion, Greece.
- KMID: 2405117
- DOI: http://doi.org/10.4266/kjccm.2017.00535
Abstract
- In mechanically ventilated patients, assisted mechanical ventilation (MV) is employed early, following the acute phase of critical illness, in order to eliminate the detrimental effects of controlled MV, most notably the development of ventilator-induced diaphragmatic dysfunction. Nevertheless, the benefits of assisted MV are often counteracted by the development of patient-ventilator dyssynchrony. Patient-ventilator dyssynchrony occurs when either the initiation and/or termination of mechanical breath is not in time agreement with the initiation and termination of neural inspiration, respectively, or if the magnitude of mechanical assist does not respond to the patient's respiratory demand. As patient-ventilator dyssynchrony has been associated with several adverse effects and can adversely influence patient outcome, every effort should be made to recognize and correct this occurrence at bedside. To detect patient-ventilator dyssynchronies, the physician should assess patient comfort and carefully inspect the pressure- and flowtime waveforms, available on the ventilator screen of all modern ventilators. Modern ventilators offer several modifiable settings to improve patient-ventilator interaction. New proportional modes of ventilation are also very helpful in improving patient-ventilator interaction.
Figure
-
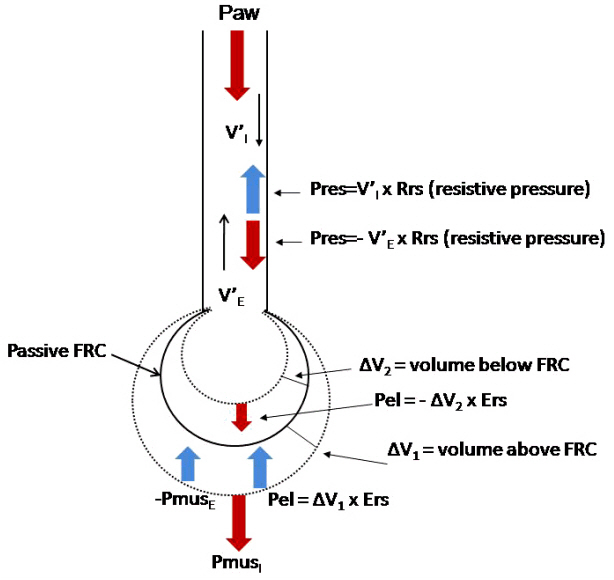
Figure 1. Schematic illustration of the respiratory system and the applied pressures. The respiratory system is presented as a balloon at passive functional residual capacity (FRC) (continuous line). Two dashed lines indicate volumes above (ΔV1) and below (ΔV2) FRC. In mechanically ventilated patients during inspiration ventilator pressure (Paw) and pressure developed by inspiratory muscles (PmusI) generate flow and the volume increases above passive FRC. The sum of these two pressures is dissipated to overcome elastic pressure (Pel), and resistive pressure (Pres). All these pressures have positive values in the equation of motion. Pressure developed by contraction of expiratory muscles (PmusE), elastic recoil pressure due to volume below passive FRC and resistive pressure due to V’E have negative values in the equation. V’I : inspiratory flow; Rrs: resistance of the respiratory system; V’E: expiratory flow; Ers: elastance of the respiratory system. Modified from Kondili et al. Br J Anaesth 2003;91:106-19, with permission of Oxford University Press [43].
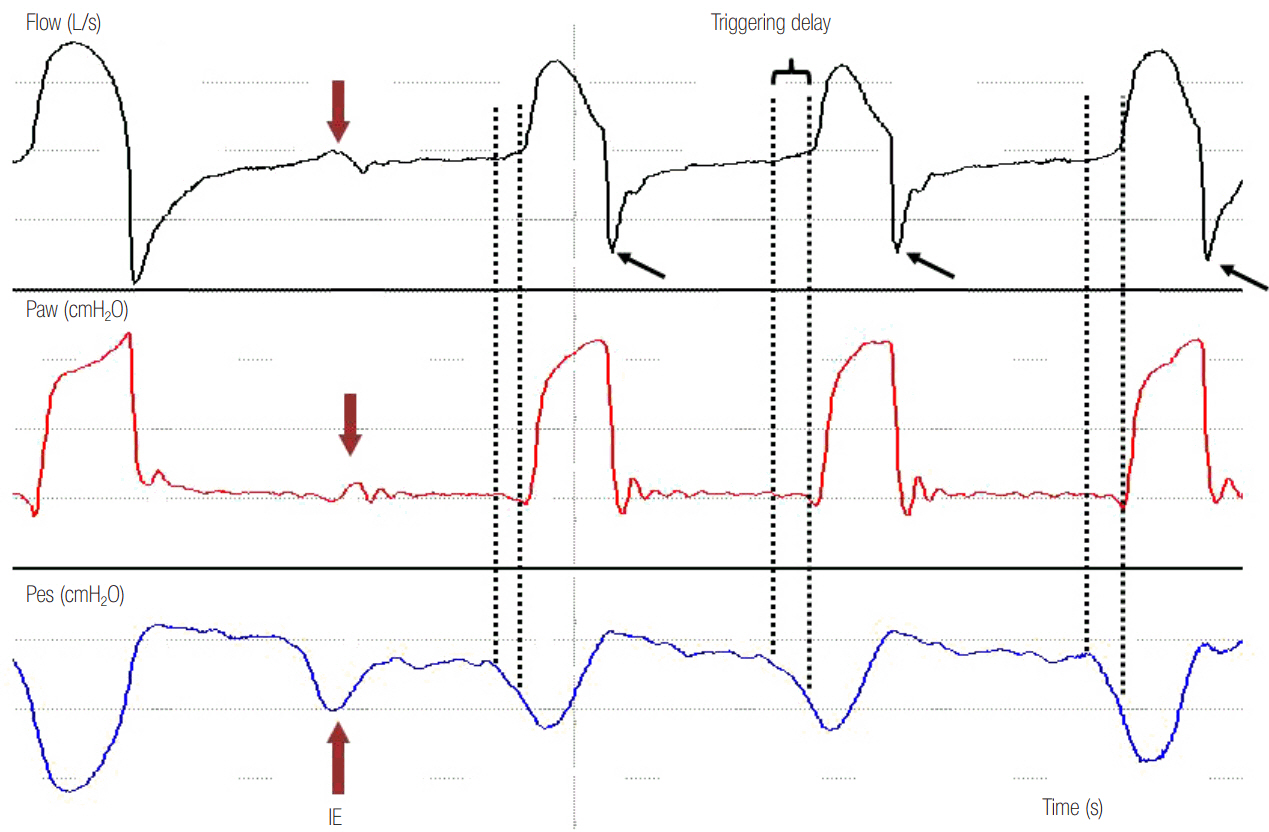
Figure 2. Airway pressure (Paw), flow and esophageal pressure (Pes) time curves in a patient ventilated with pressure support ventilation. Observe that the second decrease in Pes, which represents inspiratory effort of the patient, is not followed by a mechanical breath. This is ineffective effort (IE) during expiration and is manifested by a slight decrease in Paw associated with a simultaneous decrease in expiratory flow (red arrows). Notice that the signal of flow distortion is much clearer than the corresponding Paw change. In every mechanical breath, there is a time lag between the start of neural inspiration (first dotted line) and the start of mechanical inspiration (second dotted line). This time lag is the triggering delay. Observe the spike early in expiratory flow (black arrows) after each breath that suggests high airway resistance and long-time constant causing incomplete exhalation (flow is not zero before the next breath). Dynamic hyperinflation causes triggering delay and, combined with a relatively weaker patient effort (second Pes deflection smaller than the others) leads to ineffective triggering.
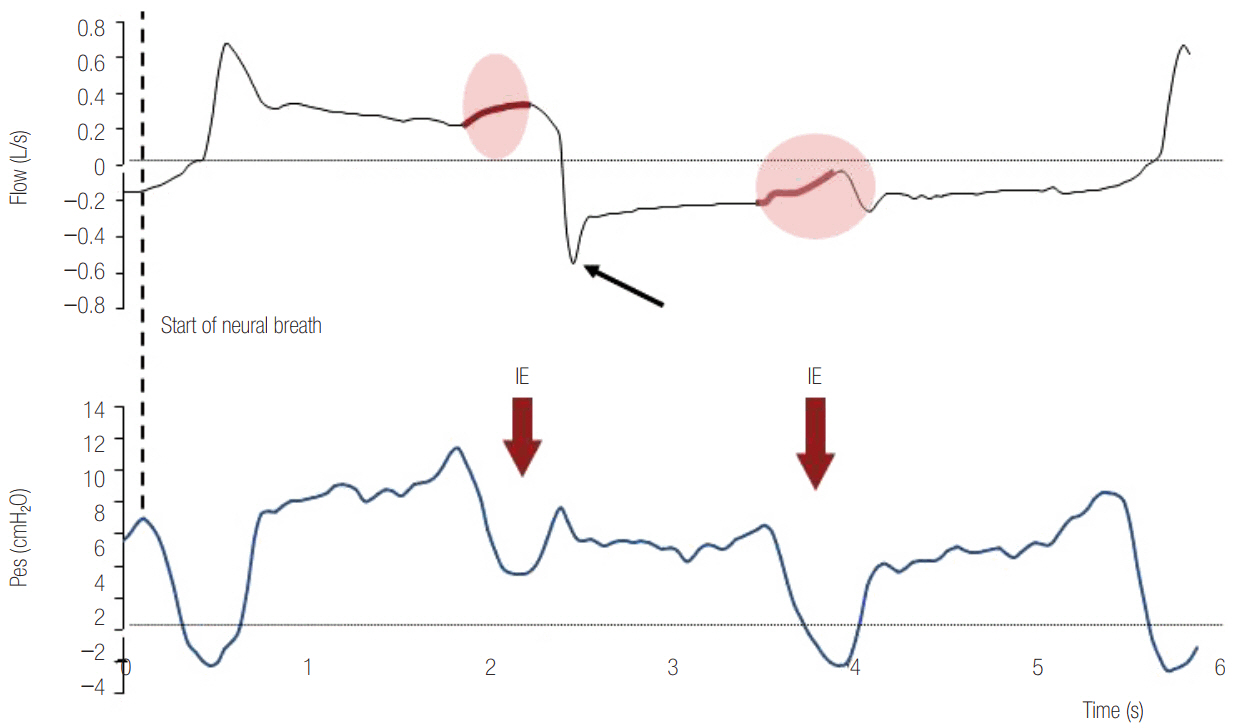
Figure 3. Flow and esophageal pressure (Pes) time curves in a patient ventilated with pressure support ventilation. The start of neural inspiration (dotted line) is indicated by a rapid decrease in Pes associated with a rapid decrease in expiratory flow (expiratory flow returns rapidly to zero line). The two subsequent patient efforts are not accompanied by a mechanical breath and represent ineffective efforts (IE, red arrows). Both can be identified by the associated flow distortion. The first IE takes place during mechanical inspiration and causes an increase in inspiratory flow waveform. The second IE happens during expiration and is manifested by a decrease in expiratory flow. The spike early in expiratory flow (black arrow) due to high airway resistance and the incomplete exhalation (flow is not zero before the next breath) are signs of dynamic hyperinflation.
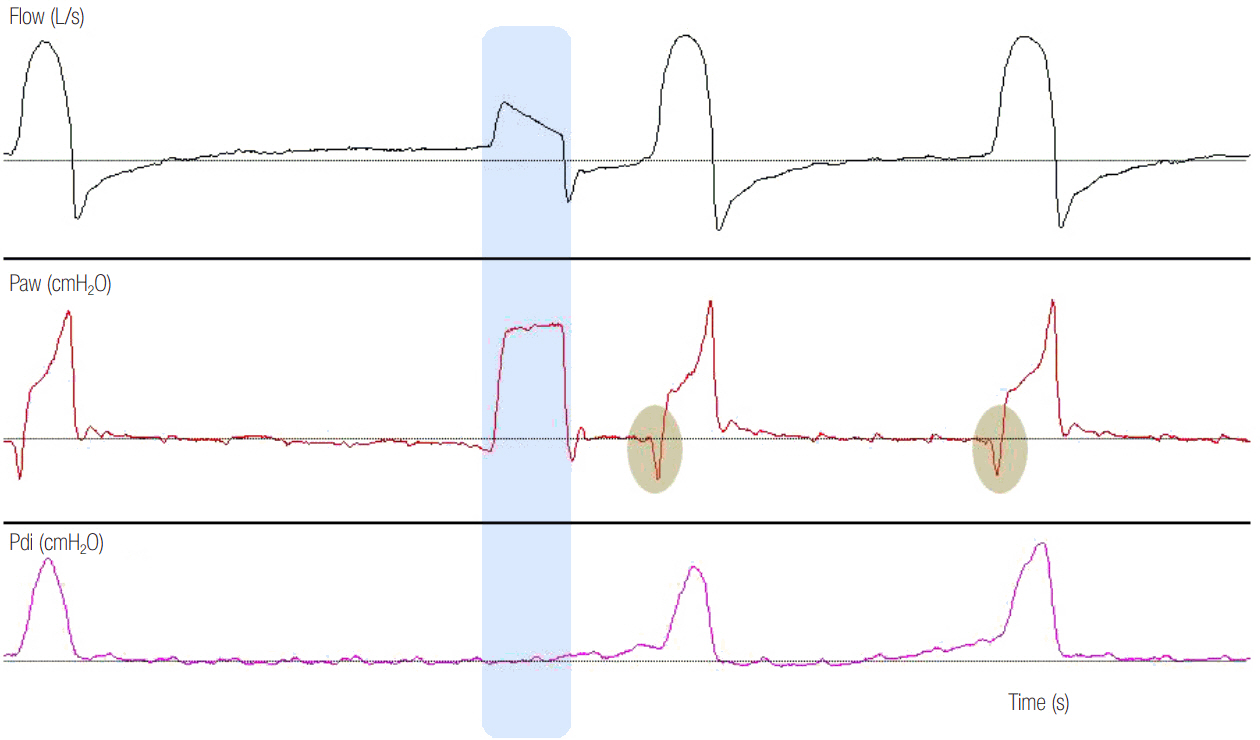
Figure 4. Airway pressure (Paw), flow and transdiaphragmatic pressure (Pdi) time curves of a patient ventilated on pressure support ventilation are illustrated. As indicated by the absence of Pdi increase, there is no inspiratory effort before the second mechanical breath (autotriggered breath, see blue shaded area). We can observe that, in comparison to patient-triggered breaths, where a decrease in Paw is observed before the start of mechanical inflation (grey shaded areas), there is no distortion in the Paw- (no decrease in Paw) and flow-time curve in the autotriggered breath. Moreover, the shape of the inspiratory flow-time curve is different compared to that of patient-triggered breaths. Notice the absence of dynamic hyperinflation in this patient (expiratory flow returns to zero after each breath).
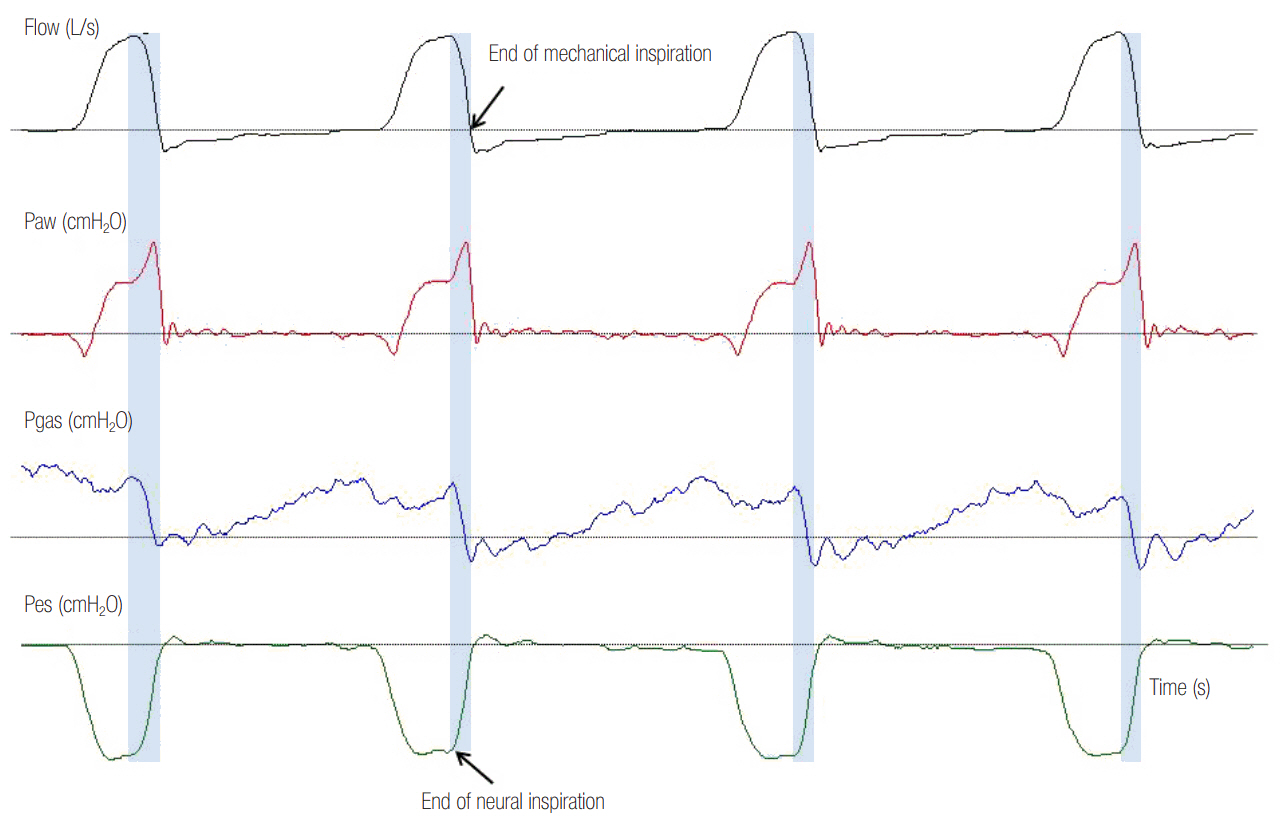
Figure 5. Delayed opening of the expiratory valve. Flow, airway pressure (Paw), gastric pressure (Pgas) and esophageal pressure (Pes) time waveforms in a patient ventilated with pressure support ventilation. There is a significant time delay (blue shaded area) between the end of neural inspiration, recognized by a rapid increase in Pes, and the end of mechanical inspiration, signified by the termination of inspiratory flow (inspiratory flow equals zero). Observe the rapid increase of Paw towards the end of mechanical inspiration, indicating inspiratory muscle relaxation.
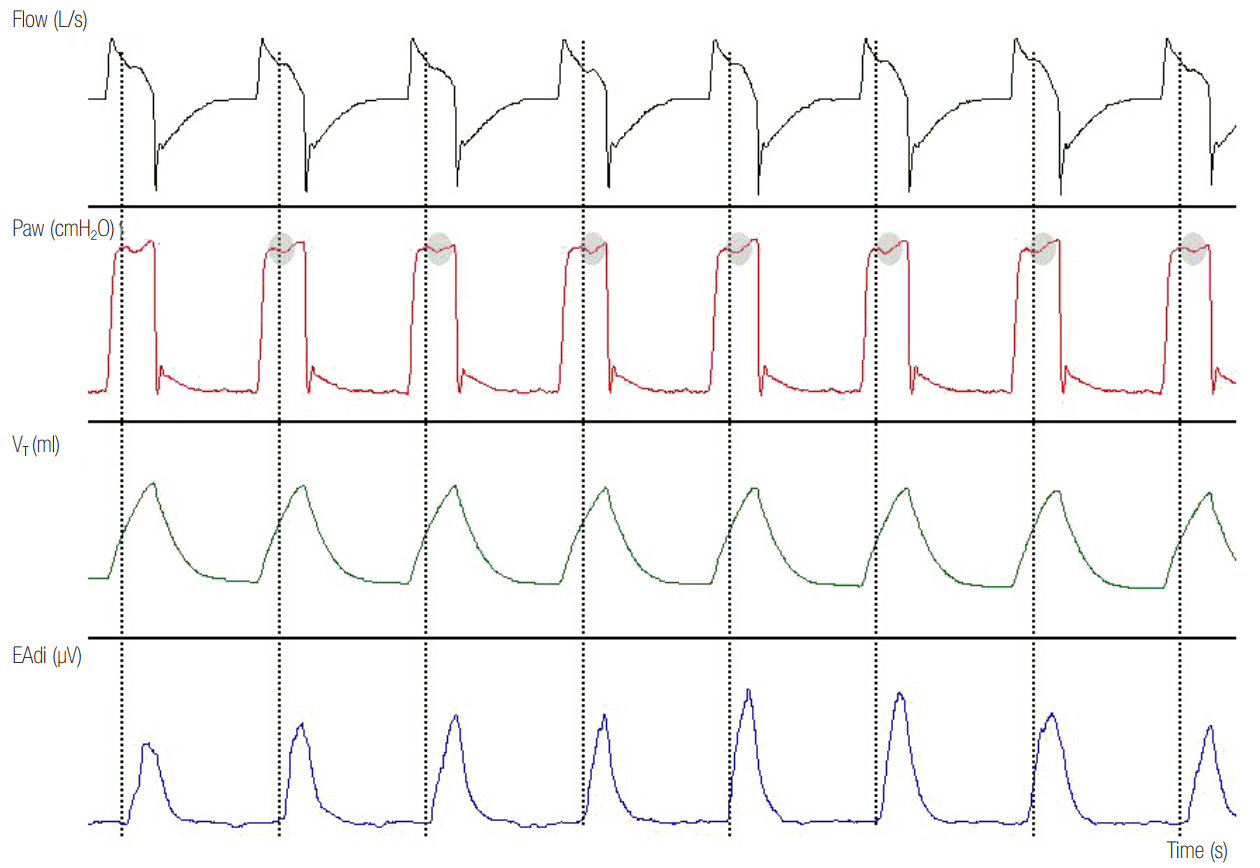
Figure 6. Reverse triggering in a patient ventilated with assist pressure control ventilation. There is an inspiratory effort of the patient (dotted lines), as evidenced by the rapid increase in electromyographic activity of the diaphragm (EAdi) after every mechanical inflation (1:1 relationship). The time interval between the initiation of mechanical and neural inspiration is fixed. Indirect evidence of patient inspiratory activity during mechanical inflation is the notch in Paw (grey shaded area). Paw: airway pressure; VT: tidal volume.
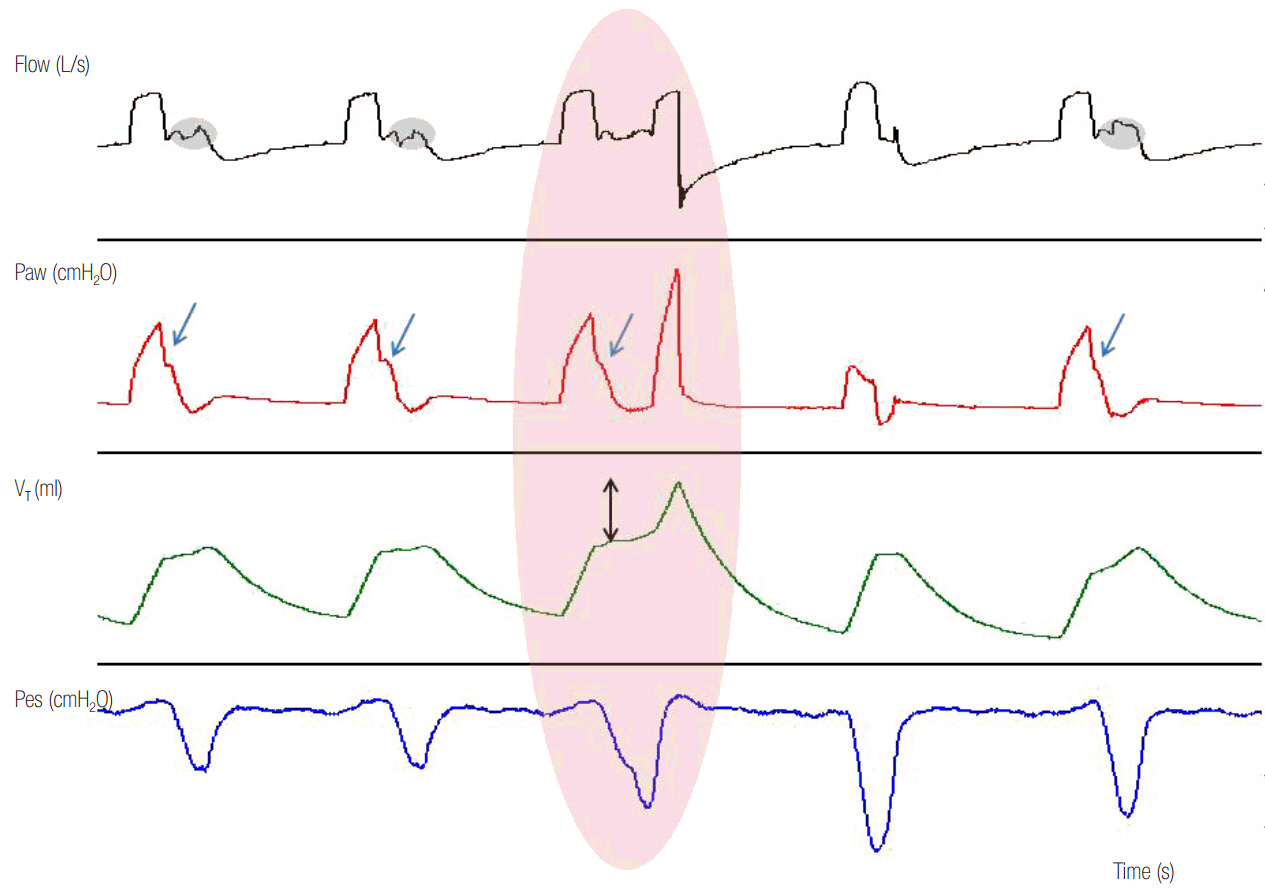
Figure 7. Reverse triggering in a patient ventilated with assist volume control ventilation. Esophageal pressure (Pes) decrease reveals patient inspiratory efforts (blue line) after every mechanical inflation in 1:1 relationship. Indirect evidence of patient inspiratory activity during mechanical inflation is the flow distortion (grey shaded area) and the disappearance (blue arrows) of plateau airway pressure (Paw) in the flow-time and Paw-time waveform, respectively. In this patient, a reverse triggered breath was strong enough to trigger the ventilator at the end of the mechanical inspiration, causing breath stacking (red shaded area). Inflated tidal volume (VT) during breath stacking increased from 444 ml to 800 ml (double arrow).
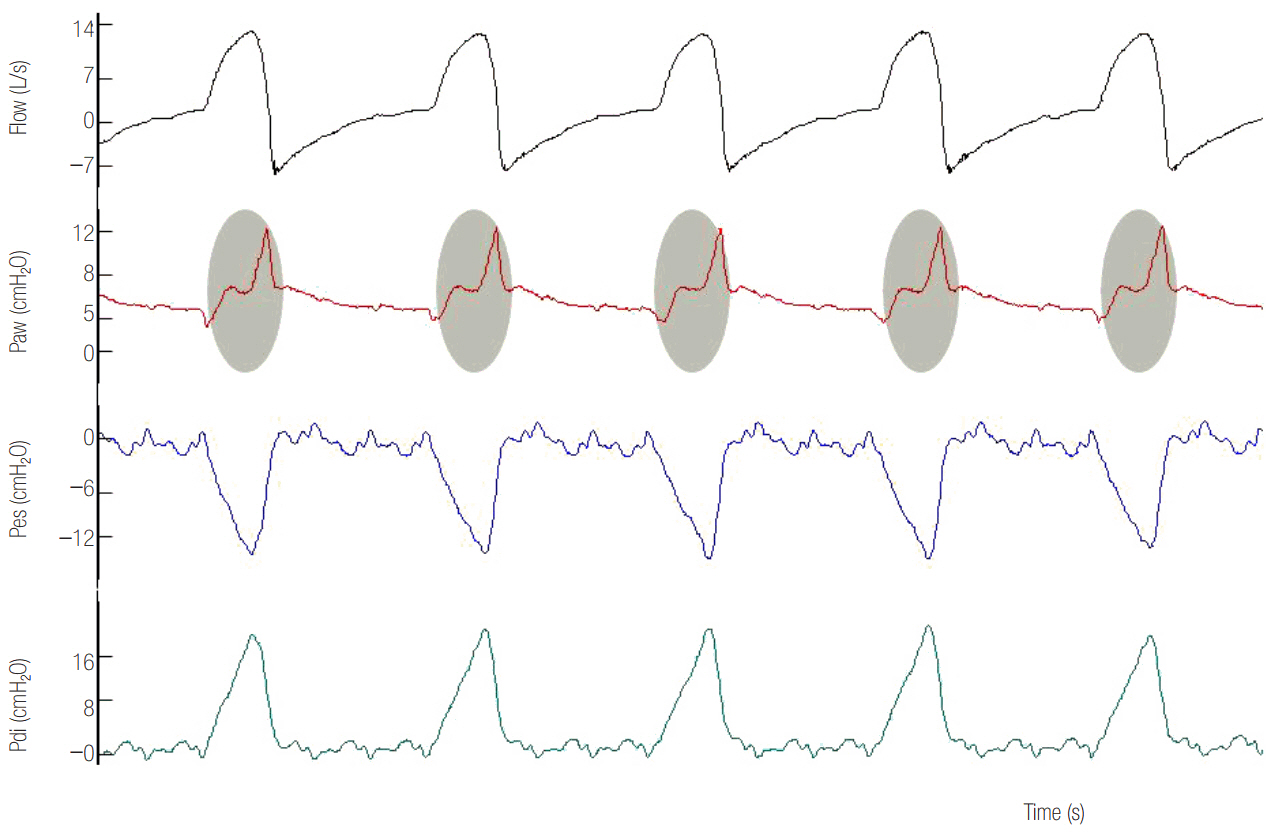
Figure 8. Flow, airway pressure (Paw), esophageal pressure (Pes) and transdiaphragmatic pressure (Pdi) time waveforms in a patient ventilated with pressure support ventilation. Observe the vigorous contraction of inspiratory muscles (Pdi increase) during the mechanical inspiration. The magnitude of this contraction causes a rounded inspiratory flow and a large decrease of Paw (gray shaded area) from the expected square-shaped form during inspiration. Rounded flow and Paw decrease are signs of low ventilator assist with respect to patients ventilator demands.
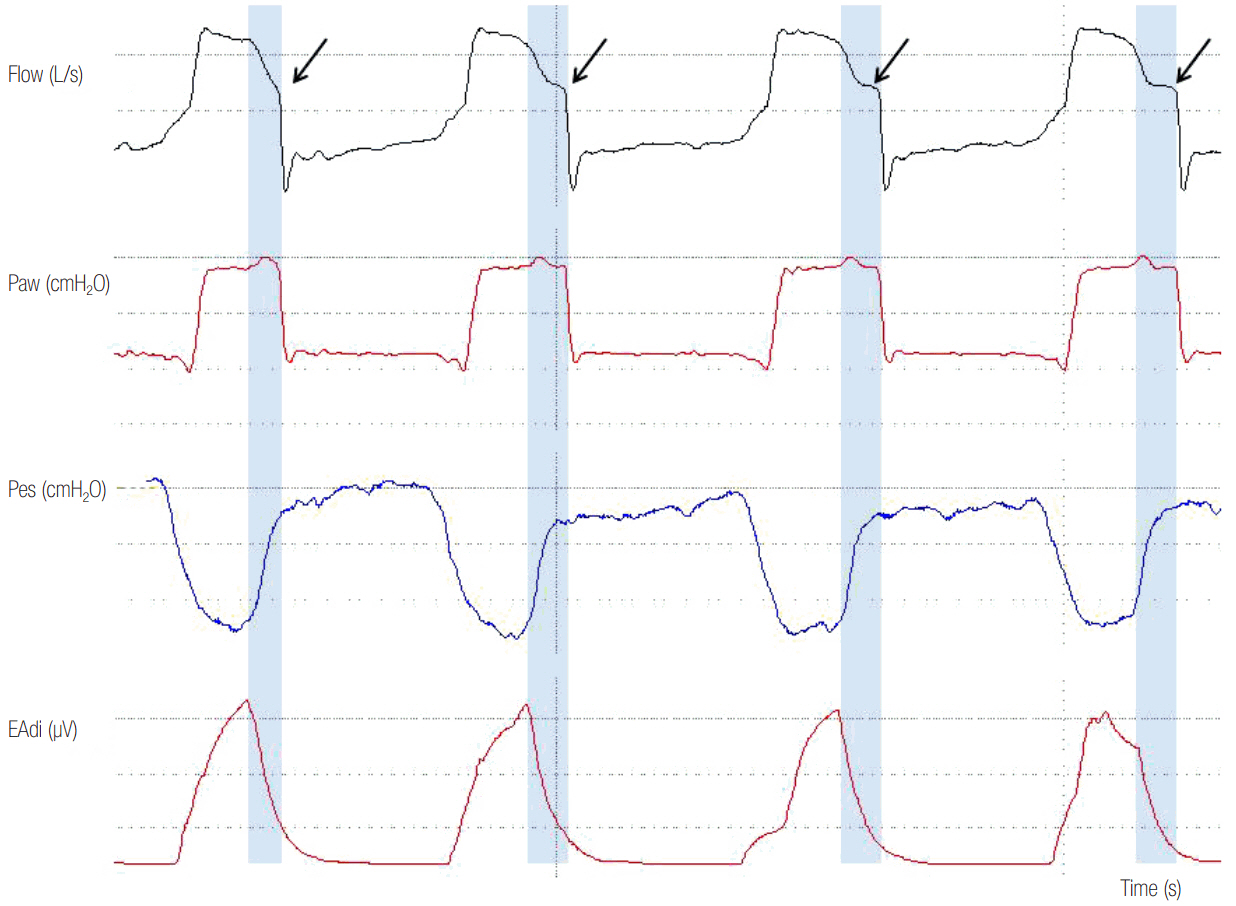
Figure 9. High assist in a patient ventilated with pressure support ventilation. Observe the square shaped airway pressure (Paw) and the abrupt decrease in inspiratory flow to flow threshold for cycling off towards the end of inspiration (arrows). There is also a significant cycling off delay (blue shaded area), seen often at high assist levels. Esophageal pressure (Pes) and electromyographic activity of the diaphragm (EAdi) decrease rapidly but mechanical inflation continues. Importantly, expiratory muscles contract during the whole expiration.
Reference
-
References
1. Petrof BJ, Jaber S, Matecki S. Ventilator-induced diaphragmatic dysfunction. Curr Opin Crit Care. 2010; 16:19–25.
Article2. Levine S, Nguyen T, Taylor N, Friscia ME, Budak MT, Rothenberg P, et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med. 2008; 358:1327–35.
Article3. Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000; 342:1471–7.
Article4. Schweickert WD, Gehlbach BK, Pohlman AS, Hall JB, Kress JP. Daily interruption of sedative infusions and complications of critical illness in mechanically ventilated patients. Crit Care Med. 2004; 32:1272–6.
Article5. Garnacho-Montero J, Madrazo-Osuna J, Garcia- Garmendia JL, Ortiz-Leyba C, Jimenez-Jimenez FJ, Barrero-Almodovar A, et al. Critical illness polyneuropathy: risk factors and clinical consequences. A cohort study in septic patients. Intensive Care Med. 2001; 27:1288–96.
Article6. Putensen C, Zech S, Wrigge H, Zinserling J, Stuber F, Von Spiegel T, et al. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med. 2001; 164:43–9.
Article7. de Wit M, Miller KB, Green DA, Ostman HE, Gennings C, Epstein SK. Ineffective triggering predicts increased duration of mechanical ventilation. Crit Care Med. 2009; 37:2740–5.
Article8. Thille AW, Rodriguez P, Cabello B, Lellouche F, Brochard L. Patient-ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med. 2006; 32:1515–22.
Article9. Blanch L, Villagra A, Sales B, Montanya J, Lucangelo U, Lujan M, et al. Asynchronies during mechanical ventilation are associated with mortality. Intensive Care Med. 2015; 41:633–41.
Article10. Bosma K, Ferreyra G, Ambrogio C, Pasero D, Mirabella L, Braghiroli A, et al. Patient-ventilator interaction and sleep in mechanically ventilated patients: pressure support versus proportional assist ventilation. Crit Care Med. 2007; 35:1048–54.
Article11. Georgopoulos D, Prinianakis G, Kondili E. Bedside waveforms interpretation as a tool to identify patient-ventilator asynchronies. Intensive Care Med. 2006; 32:34–47.
Article12. Sassoon CS, Gruer SE. Characteristics of the ventilator pressure- and flow-trigger variables. Intensive Care Med. 1995; 21:159–68.13. Aslanian P, El Atrous S, Isabey D, Valente E, Corsi D, Harf A, et al. Effects of flow triggering on breathing effort during partial ventilatory support. Am J Respir Crit Care Med. 1998; 157:135–43.
Article14. Goulet R, Hess D, Kacmarek RM. Pressure vs flow triggering during pressure support ventilation. Chest. 1997; 111:1649–53.
Article15. Prinianakis G, Kondili E, Georgopoulos D. Effects of the flow waveform method of triggering and cycling on patient-ventilator interaction during pressure support. Intensive Care Med. 2003; 29:1950–9.
Article16. Racca F, Squadrone V, Ranieri VM. Patient-ventilator interaction during the triggering phase. Respir Care Clin N Am. 2005; 11:225–45.
Article17. Slutsky AS. Mechanical ventilation: American College of Chest Physicians’ Consensus Conference. Chest. 1993; 104:1833–59.18. Prinianakis G, Kondili E, Georgopoulos D. Patient-ventilator interaction: an overview. Respir Care Clin N Am. 2005; 11:201–24.
Article19. Tobin MJ, Jubran A, Laghi F. Patient-ventilator interaction. Am J Respir Crit Care Med. 2001; 163:1059–63.
Article20. Sharshar T, Desmarais G, Louis B, Macadou G, Porcher R, Harf A, et al. Transdiaphragmatic pressure control of airway pressure support in healthy subjects. Am J Respir Crit Care Med. 2003; 168:760–9.
Article21. Sinderby C, Navalesi P, Beck J, Skrobik Y, Comtois N, Friberg S, et al. Neural control of mechanical ventilation in respiratory failure. Nat Med. 1999; 5:1433–6.
Article22. Kondili E, Xirouchaki N, Georgopoulos D. Modulation and treatment of patient-ventilator dyssynchrony. Curr Opin Crit Care. 2007; 13:84–9.
Article23. Georgopoulos DB, Anastasaki M, Katsanoulas K. Effects of mechanical ventilation on control of breathing. Monaldi Arch Chest Dis. 1997; 52:253–62.24. Brander L, Leong-Poi H, Beck J, Brunet F, Hutchison SJ, Slutsky AS, et al. Titration and implementation of neurally adjusted ventilatory assist in critically ill patients. Chest. 2009; 135:695–703.
Article25. Bonmarchand G, Chevron V, Chopin C, Jusserand D, Girault C, Moritz F, et al. Increased initial flow rate reduces inspiratory work of breathing during pressure support ventilation in patients with exacerbation of chronic obstructive pulmonary disease. Intensive Care Med. 1996; 22:1147–54.
Article26. Bonmarchand G, Chevron V, Ménard JF, Girault C, Moritz-Berthelot F, Pasquis P, et al. Effects of pressure ramp slope values on the work of breathing during pressure support ventilation in restrictive patients. Crit Care Med. 1999; 27:715–22.
Article27. Chiumello D, Pelosi P, Taccone P, Slutsky A, Gattinoni L. Effect of different inspiratory rise time and cycling off criteria during pressure support ventilation in patients recovering from acute lung injury. Crit Care Med. 2003; 31:2604–10.
Article28. Chiumello D, Pelosi P, Calvi E, Bigatello LM, Gattinoni L. Different modes of assisted ventilation in patients with acute respiratory failure. Eur Respir J. 2002; 20:925–33.
Article29. Thille AW, Cabello B, Galia F, Lyazidi A, Brochard L. Reduction of patient-ventilator asynchrony by reducing tidal volume during pressure-support ventilation. Intensive Care Med. 2008; 34:1477–86.
Article30. Leung P, Jubran A, Tobin MJ. Comparison of assisted ventilator modes on triggering, patient effort, and dyspnea. Am J Respir Crit Care Med. 1997; 155:1940–8.
Article31. Younes M, Kun J, Webster K, Roberts D. Response of ventilator-dependent patients to delayed opening of exhalation valve. Am J Respir Crit Care Med. 2002; 166:21–30.
Article32. Vaporidi K, Babalis D, Chytas A, Lilitsis E, Kondili E, Amargianitakis V, et al. Clusters of ineffective efforts during mechanical ventilation: impact on outcome. Intensive Care Med. 2017; 43:184–91.
Article33. Vitacca M, Bianchi L, Zanotti E, Vianello A, Barbano L, Porta R, et al. Assessment of physiologic variables and subjective comfort under different levels of pressure support ventilation. Chest. 2004; 126:851–9.
Article34. Nava S, Bruschi C, Rubini F, Palo A, Iotti G, Braschi A. Respiratory response and inspiratory effort during pressure support ventilation in COPD patients. Intensive Care Med. 1995; 21:871–9.
Article35. Rossi A, Polese G, Brandi G, Conti G. Intrinsic positive end-expiratory pressure (PEEPi). Intensive Care Med. 1995; 21:522–36.
Article36. Fabry B, Guttmann J, Eberhard L, Bauer T, Haberthür C, Wolff G. An analysis of desynchronization between the spontaneously breathing patient and ventilator during inspiratory pressure support. Chest. 1995; 107:1387–94.
Article37. Imanaka H, Nishimura M, Takeuchi M, Kimball WR, Yahagi N, Kumon K. Autotriggering caused by cardiogenic oscillation during flow-triggered mechanical ventilation. Crit Care Med. 2000; 28:402–7.
Article38. Hill LL, Pearl RG. Flow triggering, pressure triggering, and autotriggering during mechanical ventilation. Crit Care Med. 2000; 28:579–81.
Article39. Carteaux G, Lyazidi A, Cordoba-Izquierdo A, Vignaux L, Jolliet P, Thille AW, et al. Patient-ventilator asynchrony during noninvasive ventilation: a bench and clinical study. Chest. 2012; 142:367–76.40. Sassoon CS, Zhu E, Caiozzo VJ. Assist-control mechanical ventilation attenuates ventilator-induced diaphragmatic dysfunction. Am J Respir Crit Care Med. 2004; 170:626–32.
Article41. Du HL, Yamada Y. Expiratory asynchrony. Respir Care Clin N Am. 2005; 11:265–80.
Article42. Prinianakis G, Plataki M, Kondili E, Klimathianaki M, Vaporidi K, Georgopoulos D. Effects of relaxation of inspiratory muscles on ventilator pressure during pressure support. Intensive Care Med. 2008; 34:70–4.43. Kondili E, Prinianakis G, Georgopoulos D. Patient-ventilator interaction. Br J Anaesth. 2003; 91:106–19.
Article44. Yamada Y, Du HL. Analysis of the mechanisms of expiratory asynchrony in pressure support ventilation: a mathematical approach. J Appl Physiol (1985). 2000; 88:2143–50.45. Akoumianaki E, Lyazidi A, Rey N, Matamis D, Perez- Martinez N, Giraud R, et al. Mechanical ventilation-induced reverse-triggered breaths: a frequently unrecognized form of neuromechanical coupling. Chest. 2013; 143:927–38.46. Simon PM, Habel AM, Daubenspeck JA, Leiter JC. Vagal feedback in the entrainment of respiration to mechanical ventilation in sleeping humans. J Appl Physiol (1985). 2000; 89:760–9.
Article47. Simon PM, Zurob AS, Wies WM, Leiter JC, Hubmayr RD. Entrainment of respiration in humans by periodic lung inflations: effect of state and CO(2). Am J Respir Crit Care Med. 1999; 160:950–60.48. Meza S, Mendez M, Ostrowski M, Younes M. Susceptibility to periodic breathing with assisted ventilation during sleep in normal subjects. J Appl Physiol (1985). 1998; 85:1929–40.49. Tobin MJ. Monitoring of pressure, flow, and volume during mechanical ventilation. Respir Care. 1992; 37:1081–96.50. Jubran A, Van de Graaff WB, Tobin MJ. Variability of patient-ventilator interaction with pressure support ventilation in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1995; 152:129–36.
Article51. Terzi N, Pelieu I, Guittet L, Ramakers M, Seguin A, Daubin C, et al. Neurally adjusted ventilatory assist in patients recovering spontaneous breathing after acute respiratory distress syndrome: physiological evaluation. Crit Care Med. 2010; 38:1830–7.
Article52. Spahija J, de Marchie M, Albert M, Bellemare P, Delisle S, Beck J, et al. Patient-ventilator interaction during pressure support ventilation and neurally adjusted ventilatory assist. Crit Care Med. 2010; 38:518–26.
Article53. Xirouchaki N, Kondili E, Vaporidi K, Xirouchakis G, Klimathianaki M, Gavriilidis G, et al. Proportional assist ventilation with load-adjustable gain factors in critically ill patients: comparison with pressure support. Intensive Care Med. 2008; 34:2026–34.
Article54. Piquilloud L, Vignaux L, Bialais E, Roeseler J, Sottiaux T, Laterre PF, et al. Neurally adjusted ventilatory assist improves patient-ventilator interaction. Intensive Care Med. 2011; 37:263–71.
Article55. Kondili E, Prinianakis G, Alexopoulou C, Vakouti E, Klimathianaki M, Georgopoulos D. Respiratory load compensation during mechanical ventilation: proportional assist ventilation with load-adjustable gain factors versus pressure support. Intensive Care Med. 2006; 32:692–9.56. Lecomte F, Brander L, Jalde F, Beck J, Qui H, Elie C, et al. Physiological response to increasing levels of neurally adjusted ventilatory assist (NAVA). Respir Physiol Neurobiol. 2009; 166:117–24.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Impact of Left Bundle Branch Block on Left Atrial Dyssynchrony and Its Relationship to Left Ventricular Diastolic Function in Patients with Heart Failure and Dilated Cardiomyopathy
- Left Ventricular Dyssynchrony in Patients Showing Diastolic Dysfunction without Overt Symptoms of Heart Failure
- Ventricular dyssynchrony in patients with permanent pacemaker
- Clinical Implication of Mechanical Dyssynchrony in Heart Failure
- Does the " Curare Cleft " on the Capnogram always mean that the Patient is in Need of Relaxant ?
