Advances in Intravascular Imaging: New Insights into the Vulnerable Plaque from Imaging Studies
- Affiliations
-
- 1Department of Cardiovascular Medicine, Tsuchiura Kyodo General Hospital, Tsuchiura, Japan.
- 2Cardiology Division, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA. ijang@mgh.harvard.edu
- 3Division of Cardiology, Kyung-Hee University Hospital, Seoul, Korea.
- KMID: 2405041
- DOI: http://doi.org/10.4070/kcj.2017.0182
Abstract
- The term "vulnerable plaque" denotes the plaque characteristics that are susceptible to coronary thrombosis. Previous post-mortem studies proposed 3 major mechanisms of coronary thrombosis: plaque rupture, plaque erosion, and calcified nodules. Of those, characteristics of rupture-prone plaque have been extensively studied. Pathology studies have identified the features of rupture-prone plaque including thin fibrous cap, large necrotic core, expansive vessel remodeling, inflammation, and neovascularization. Intravascular imaging modalities have emerged as adjunctive tools of angiography to identify vulnerable plaques. Multiple devices have been introduced to catheterization laboratories to date, including intravascular ultrasound (IVUS), virtual-histology IVUS, optical coherence tomography (OCT), coronary angioscopy, and near-infrared spectroscopy. With the use of these modalities, our understanding of vulnerable plaque has rapidly grown over the past several decades. One of the goals of intravascular imaging is to better predict and prevent future coronary events, for which prospective observational data is still lacking. OCT delineates microstructures of plaques, whereas IVUS visualizes macroscopic vascular structures. Specifically, plaque erosion, which has been underestimated in clinical practice, is gaining an interest due to the potential of OCT to make an in vivo diagnosis. Another potential future avenue for intravascular imaging is its use to guide treatment. Feasibility of tailored therapy for acute coronary syndromes (ACS) guided by OCT is under investigation. If it is proven to be effective, it may potentially lead to major shift in the management of millions of patients with ACS every year.
Keyword
MeSH Terms
Figure
-

Figure 1 A lesion with a necrotic core assessed by VH-IVUS. A fibroatheroma was imaged by grey-scale IVUS (upper row) and VH-IVUS (lower row). VH-IVUS categorizes the tissue into DC, FT, FF, or NC by processing the radiofrequency data of IVUS. In general, a plaque containing >10% of NC is defined as fibroatheroma. When NC is adjacent to the lumen >30 degrees of circumferences on 3 consecutive frames, fibroatherma is defined as VH-TCFA, as proposed in the PROSPECT study. The lesion in the third column contains >10% of NC, but the angle of NC adjacent to the lumen is not >30 degrees. Therefore, the lesion is defined as ThCFA. DC = dense calcium; FT = fibrous tissue; FF = fibrofatty tissue; IVUS = intravascular ultrasound; NC = necrotic core; PROSPECT = Providing Regional Observations to Study Predictors of Events in the Coronary Tree; ThCFA = thick-cap fibroatheroma; VH-IVUS = virtual-histology intravascular ultrasound; VH-TCFA = virtual-histology-derived thin-cap fibroatheroma.
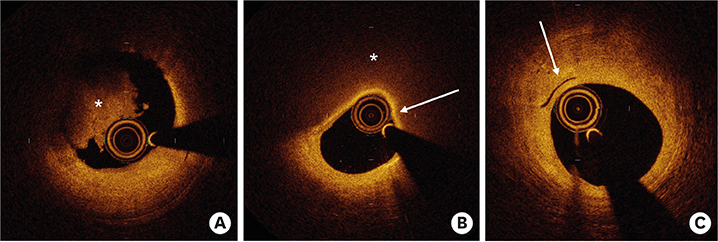
Figure 2 Typical OCT findings representing vulnerable plaques. (A) shows intraluminal thrombus characterized by a mass (*) attached to the wall (9–12 o'clock). (B) shows TCFA characterized by a signal poor region (*) with a thin, signal rich band (white arrow) on the luminal side. (C) shows a fibrous plaque with neovascularization characterized by a tubuloluminal, signal lucent structure (white arrow) within the plaque. OCT = optical coherence tomography; TCFA = thin cap fibroatheroma.
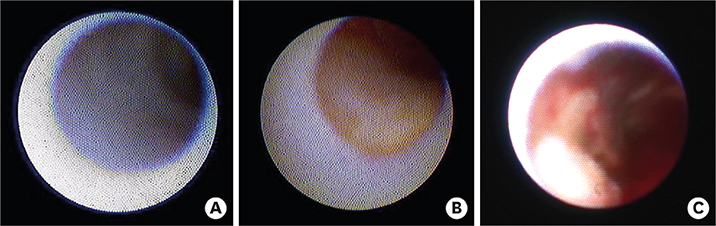
Figure 3 Coronary plaques imaged by angioscopy. Angioscopy allows direct visualization of coronary plaques surface from the luminal side. Plaque characteristics is categorized by color grading: white (grade 0); light yellow (grade 1); yellow (grade 2); or intensive yellow (grade 3). (A) shows white plaque (grade 0) and (B) shows yellow plaque (grade 2). In addition to the color grade, presence of thrombus and plaque disruption can be visualized by angioscopy. (C) shows a plaque rupture with red thrombus.
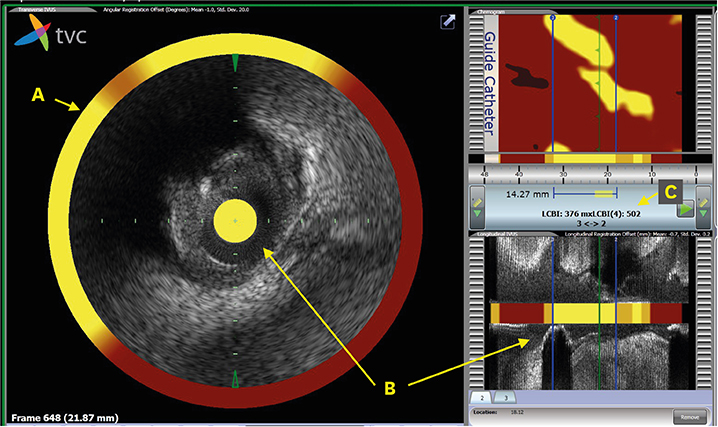
Figure 4 A lipid-rich plaque imaged by NIRS. A culprit lesion of NSTEMI was examined by NIRS co-registered with grey-scale IVUS. NIRS provides a probability of the presence of lipid ranging from 0 to 1.0 for each pixel occupying 0.1 mm and 1 degree, which is indicated on a map of lumen surface called “chemogram” (Right upper panel). The information of the probability is superimposed on the rim of grey-scale IVUS (A). In the center of grey-scale IVUS and in the right lower panel, “block chemogram” which summarizes the probability value of each 2-mm segment is shown (B). Numbers of pixels of which the probability is >0.6 is expressed as permil, and called LCBI. Max LCBI4mm is generally used as an indicator of lipid volume (C). IVUS = intravascular ultrasound; LCBI = lipid core burden index; Max LCBI4mm = Maximal LCBI value within a 4 mm-segment; NIRS = near-infrared spectroscopy; NSTEMI = non-ST-elevation myocardial infarction.

Figure 5 Positive remodeling. EEM area can be measured with IVUS. RI is calculated as the ratio of lesion EEM area divided by that of reference site. Threshold of RI for positive remodeling varies among different studies. In previous IVUS studies, RI >1.05 or 1.00 were predominantly used for the definition of positive remodeling. In this figure, RI is 1.37, which indicates significant positive remodeling. EEM = external elastic membrane; IVUS = intravascular ultrasound; RI = remodeling index.
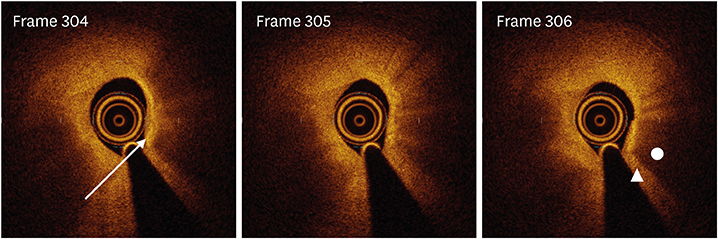
Figure 6 Macrophage accumulation. Three consecutive frames of a plaque showing macrophage accumulation. Macrophage accumulation is identified by punctate or linear high-signal intensities accompanied by heterogenic shadow (white arrow, frame 304), which cast on the deeper layer of intima. Heterogenic shadow is characterized by frame-by-frame variability (frame 304–306) and sharp radial border between plaque density (triangle, frame 306) and a shadow density (circle, frame 306) within the plaque.
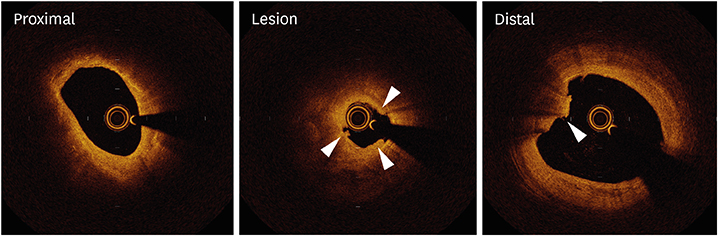
Figure 7 Plaque erosion on OCT. OCT images of a culprit lesion of NSTEMI show “definite” erosion. Definite erosion is defined by OCT as having intact fibrous cap underneath thrombi (arrowheads) that do not preclude plaque characterization behind the thrombus. NSTEMI = non-ST-elevation myocardial infarction; OCT = optical coherence tomography.
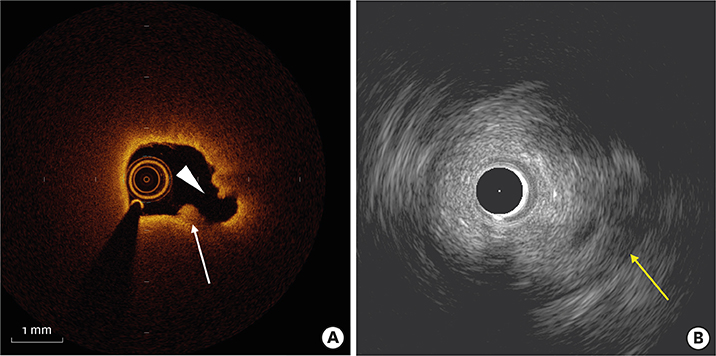
Figure 8 Plaque rupture imaged by OCT and IVUS. Plaque rupture in a culprit lesion of STEMI is imaged by OCT (A) and IVUS (B). OCT clearly visualizes disruption of fibrous cap (arrow head) and a thrombus attached to the lumen (white arrow), however circumferential lipid precludes visualization of entire vessel wall. In contrast, IVUS delineate medial layer (yellow arrow) beyond the plaque, whereas microstructure beside the lumen such as a thrombus and plaque rupture are not detectable. IVUS = intravascular ultrasound; OCT = optical coherence tomography; STEMI = ST-segment elevation myocardial infarction.
Reference
-
1. Falk E. Plaque rupture with severe pre-existing stenosis precipitating coronary thrombosis. Characteristics of coronary atherosclerotic plaques underlying fatal occlusive thrombi. Br Heart J. 1983; 50:127–134.
Article2. Friedman M, Van den Bovenkamp GJ. Role of thrombus in plaque formation in the human diseased coronary artery. Br J Exp Pathol. 1966; 47:550–557.3. Willerson JT, Campbell WB, Winniford MD, et al. Conversion from chronic to acute coronary artery disease: speculation regarding mechanisms. Am J Cardiol. 1984; 54:1349–1354.
Article4. Davies MJ. A macro and micro view of coronary vascular insult in ischemic heart disease. Circulation. 1990; 82:II38–II46.5. Davies MJ, Thomas AC. Plaque fissuring--the cause of acute myocardial infarction, sudden ischaemic death, and crescendo angina. Br Heart J. 1985; 53:363–373.
Article6. Libby P, Theroux P. Pathophysiology of coronary artery disease. Circulation. 2005; 111:3481–3488.
Article7. Muller JE, Abela GS, Nesto RW, Tofler GH. Triggers, acute risk factors and vulnerable plaques: the lexicon of a new frontier. J Am Coll Cardiol. 1994; 23:809–813.
Article8. Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol. 2000; 20:1262–1275.9. Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: part I. Circulation. 2003; 108:1664–1672.10. Arbustini E, Dal Bello B, Morbini P, et al. Plaque erosion is a major substrate for coronary thrombosis in acute myocardial infarction. Heart. 1999; 82:269–272.
Article11. Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: part II. Circulation. 2003; 108:1772–1778.12. Moreno PR, Purushothaman KR, Fuster V, et al. Plaque neovascularization is increased in ruptured atherosclerotic lesions of human aorta: implications for plaque vulnerability. Circulation. 2004; 110:2032–2038.13. Kolodgie FD, Burke AP, Farb A, et al. The thin-cap fibroatheroma: a type of vulnerable plaque: the major precursor lesion to acute coronary syndromes. Curr Opin Cardiol. 2001; 16:285–292.
Article14. Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006; 47:C13–8.
Article15. Kato K, Yonetsu T, Kim SJ, et al. Nonculprit plaques in patients with acute coronary syndromes have more vulnerable features compared with those with non-acute coronary syndromes: a 3-vessel optical coherence tomography study. Circ Cardiovasc Imaging. 2012; 5:433–440.
Article16. García-García HM, Mintz GS, Lerman A, et al. Tissue characterisation using intravascular radiofrequency data analysis: recommendations for acquisition, analysis, interpretation and reporting. EuroIntervention. 2009; 5:177–189.
Article17. Sathyanarayana S, Carlier S, Li W, Thomas L. Characterisation of atherosclerotic plaque by spectral similarity of radiofrequency intravascular ultrasound signals. EuroIntervention. 2009; 5:133–139.
Article18. Okubo M, Kawasaki M, Ishihara Y, et al. Tissue characterization of coronary plaques: comparison of integrated backscatter intravascular ultrasound with virtual histology intravascular ultrasound. Circ J. 2008; 72:1631–1639.19. Garcìa-Garcìa HM, Gogas BD, Serruys PW, Bruining N. IVUS-based imaging modalities for tissue characterization: similarities and differences. Int J Cardiovasc Imaging. 2011; 27:215–224.
Article20. Jang IK, Bouma BE, Kang DH, et al. Visualization of coronary atherosclerotic plaques in patients using optical coherence tomography: comparison with intravascular ultrasound. J Am Coll Cardiol. 2002; 39:604–609.
Article21. Prati F, Guagliumi G, Mintz GS, et al. Expert review document part 2: methodology, terminology and clinical applications of optical coherence tomography for the assessment of interventional procedures. Eur Heart J. 2012; 33:2513–2520.
Article22. Tearney GJ, Regar E, Akasaka T, et al. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: a report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J Am Coll Cardiol. 2012; 59:1058–1072.23. Yabushita H, Bouma BE, Houser SL, et al. Characterization of human atherosclerosis by optical coherence tomography. Circulation. 2002; 106:1640–1645.
Article24. Jang IK, Tearney GJ, MacNeill B, et al. In vivo characterization of coronary atherosclerotic plaque by use of optical coherence tomography. Circulation. 2005; 111:1551–1555.
Article25. Kume T, Akasaka T, Kawamoto T, et al. Assessment of coronary arterial plaque by optical coherence tomography. Am J Cardiol. 2006; 97:1172–1175.
Article26. Kume T, Akasaka T, Kawamoto T, et al. Assessment of coronary arterial thrombus by optical coherence tomography. Am J Cardiol. 2006; 97:1713–1717.
Article27. Mizuno K, Satomura K, Miyamoto A, et al. Angioscopic evaluation of coronary-artery thrombi in acute coronary syndromes. N Engl J Med. 1992; 326:287–291.
Article28. Mizuno K, Miyamoto A, Satomura K, et al. Angioscopic coronary macromorphology in patients with acute coronary disorders. Lancet. 1991; 337:809–812.
Article29. Burke AP, Farb A, Malcom GT, Liang YH, Smialek J, Virmani R. Coronary risk factors and plaque morphology in men with coronary disease who died suddenly. N Engl J Med. 1997; 336:1276–1282.
Article30. Kume T, Akasaka T, Kawamoto T, et al. Measurement of the thickness of the fibrous cap by optical coherence tomography. Am Heart J. 2006; 152:755.e1–755.e4.
Article31. Yonetsu T, Kakuta T, Lee T, et al. In vivo critical fibrous cap thickness for rupture-prone coronary plaques assessed by optical coherence tomography. Eur Heart J. 2011; 32:1251–1259.
Article32. Burke AP, Kolodgie FD, Farb A, et al. Healed plaque ruptures and sudden coronary death: evidence that subclinical rupture has a role in plaque progression. Circulation. 2001; 103:934–940.33. Tian J, Ren X, Vergallo R, et al. Distinct morphological features of ruptured culprit plaque for acute coronary events compared to those with silent rupture and thin-cap fibroatheroma: a combined optical coherence tomography and intravascular ultrasound study. J Am Coll Cardiol. 2014; 63:2209–2216.34. Stone GW, Maehara A, Lansky AJ, et al. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011; 364:226–235.
Article35. Maehara A, Cristea E, Mintz GS, et al. Definitions and methodology for the grayscale and radiofrequency intravascular ultrasound and coronary angiographic analyses. JACC Cardiovasc Imaging. 2012; 5:S1–S9.
Article36. Brown AJ, Obaid DR, Costopoulos C, et al. Direct comparison of virtual-histology intravascular ultrasound and optical coherence tomography imaging for identification of thin-cap fibroatheroma. Circ Cardiovasc Imaging. 2015; 8:e003487.
Article37. Uemura S, Ishigami K, Soeda T, et al. Thin-cap fibroatheroma and microchannel findings in optical coherence tomography correlate with subsequent progression of coronary atheromatous plaques. Eur Heart J. 2012; 33:78–85.
Article38. Takano M, Jang IK, Inami S, et al. In vivo comparison of optical coherence tomography and angioscopy for the evaluation of coronary plaque characteristics. Am J Cardiol. 2008; 101:471–476.
Article39. Mintz GS, Nissen SE, Anderson WD, et al. American College of Cardiology Clinical Expert Consensus Document on standards for acquisition, measurement and reporting of intravascular ultrasound studies (IVUS). A report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol. 2001; 37:1478–1492.40. Nissen SE, Nicholls SJ, Sipahi I, et al. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA. 2006; 295:1556–1565.41. Takayama T, Hiro T, Yamagishi M, et al. Effect of rosuvastatin on coronary atheroma in stable coronary artery disease: multicenter coronary atherosclerosis study measuring effects of rosuvastatin using intravascular ultrasound in Japanese subjects (COSMOS). Circ J. 2009; 73:2110–2117.42. Nicholls SJ, Puri R, Anderson T, et al. Effect of evolocumab on progression of coronary disease in statin-treated patients: the GLAGOV Randomized Clinical Trial. JAMA. 2016; 316:2373–2384.43. Xing L, Higuma T, Wang Z, et al. Clinical significance of lipid-rich plaque detected by optical coherence tomography: a 4-year follow-up study. J Am Coll Cardiol. 2017; 69:2502–2513.44. Davies MJ, Richardson PD, Woolf N, Katz DR, Mann J. Risk of thrombosis in human atherosclerotic plaques: role of extracellular lipid, macrophage, and smooth muscle cell content. Br Heart J. 1993; 69:377–381.
Article45. van der Wal AC, Becker AE, van der Loos CM, Das PK. Site of intimal rupture or erosion of thrombosed coronary atherosclerotic plaques is characterized by an inflammatory process irrespective of the dominant plaque morphology. Circulation. 1994; 89:36–44.
Article46. Nathan CF, Murray HW, Cohn ZA. The macrophage as an effector cell. N Engl J Med. 1980; 303:622–626.
Article47. Tearney GJ, Yabushita H, Houser SL, et al. Quantification of macrophage content in atherosclerotic plaques by optical coherence tomography. Circulation. 2003; 107:113–119.
Article48. MacNeill BD, Jang IK, Bouma BE, et al. Focal and multi-focal plaque macrophage distributions in patients with acute and stable presentations of coronary artery disease. J Am Coll Cardiol. 2004; 44:972–979.
Article49. Vergallo R, Papafaklis MI, Yonetsu T, et al. Endothelial shear stress and coronary plaque characteristics in humans: combined frequency-domain optical coherence tomography and computational fluid dynamics study. Circ Cardiovasc Imaging. 2014; 7:905–911.50. Phipps JE, Hoyt T, Vela D, et al. Diagnosis of thin-capped fibroatheromas in intravascular optical coherence tomography images: effects of light scattering. Circ Cardiovasc Interv. 2016; 9:e003163.
Article51. Kini AS, Vengrenyuk Y, Yoshimura T, et al. Fibrous cap thickness by optical coherence tomography in vivo. J Am Coll Cardiol. 2017; 69:644–657.52. Kume T, Okura H, Yamada R, et al. Detection of plaque neovascularization by optical coherence tomography: ex vivo feasibility study and in vivo observation in patients with angina pectoris. J Invasive Cardiol. 2016; 28:17–22.53. Kumamoto M, Nakashima Y, Sueishi K. Intimal neovascularization in human coronary atherosclerosis: its origin and pathophysiological significance. Hum Pathol. 1995; 26:450–456.
Article54. Gössl M, Versari D, Hildebrandt HA, et al. Segmental heterogeneity of vasa vasorum neovascularization in human coronary atherosclerosis. JACC Cardiovasc Imaging. 2010; 3:32–40.
Article55. Kitabata H, Tanaka A, Kubo T, et al. Relation of microchannel structure identified by optical coherence tomography to plaque vulnerability in patients with coronary artery disease. Am J Cardiol. 2010; 105:1673–1678.
Article56. Taruya A, Tanaka A, Nishiguchi T, et al. Vasa vasorum restructuring in human atherosclerotic plaque vulnerability: a clinical optical coherence tomography study. J Am Coll Cardiol. 2015; 65:2469–2477.57. Kubo T, Imanishi T, Takarada S, et al. Assessment of culprit lesion morphology in acute myocardial infarction: ability of optical coherence tomography compared with intravascular ultrasound and coronary angioscopy. J Am Coll Cardiol. 2007; 50:933–939.58. Jia H, Abtahian F, Aguirre AD, et al. In vivo diagnosis of plaque erosion and calcified nodule in patients with acute coronary syndrome by intravascular optical coherence tomography. J Am Coll Cardiol. 2013; 62:1748–1758.59. Higuma T, Soeda T, Abe N, et al. A combined optical coherence tomography and intravascular ultrasound study on plaque rupture, plaque erosion, and calcified nodule in patients with ST-segment elevation myocardial infarction: incidence, morphologic characteristics, and outcomes after percutaneous coronary intervention. JACC Cardiovasc Interv. 2015; 8:1166–1176.60. Hu S, Yonetsu T, Jia H, et al. Residual thrombus pattern in patients with ST-segment elevation myocardial infarction caused by plaque erosion versus plaque rupture after successful fibrinolysis: an optical coherence tomography study. J Am Coll Cardiol. 2014; 63:1336–1338.61. Jia H, Dai J, Hou J, et al. Effective anti-thrombotic therapy without stenting: intravascular optical coherence tomography-based management in plaque erosion (the EROSION study). Eur Heart J. 2017; 38:792–800.
Article62. Lee JB, Mintz GS, Lisauskas JB, et al. Histopathologic validation of the intravascular ultrasound diagnosis of calcified coronary artery nodules. Am J Cardiol. 2011; 108:1547–1551.
Article63. Xu Y, Mintz GS, Tam A, et al. Prevalence, distribution, predictors, and outcomes of patients with calcified nodules in native coronary arteries: a 3-vessel intravascular ultrasound analysis from Providing Regional Observations to Study Predictors of Events in the Coronary Tree (PROSPECT). Circulation. 2012; 126:537–545.64. Lee T, Mintz GS, Matsumura M, et al. Prevalence, predictors, and clinical presentation of a calcified nodule as assessed by optical coherence tomography. JACC Cardiovasc Imaging. 2017; 10:883–891.
Article65. Qian D, Bottomley PA. High-resolution intravascular magnetic resonance quantification of atherosclerotic plaque at 3T. J Cardiovasc Magn Reson. 2012; 14:20.
Article66. Jaffer FA, Calfon MA, Rosenthal A, et al. Two-dimensional intravascular near-infrared fluorescence molecular imaging of inflammation in atherosclerosis and stent-induced vascular injury. J Am Coll Cardiol. 2011; 57:2516–2526.
Article67. Li BH, Leung AS, Soong A, et al. Hybrid intravascular ultrasound and optical coherence tomography catheter for imaging of coronary atherosclerosis. Catheter Cardiovasc Interv. 2013; 81:494–507.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nuclear Molecular Imaging for Vulnerable Atherosclerotic Plaques
- Multimodal intravascular photoacoustic and ultrasound imaging
- Diagnostic and Therapeutic Approach of Carotid and Cerebrovascular Plaque on the Basis of Vessel Imaging
- Recent Advances in the Development of PET/SPECT Probes for Atherosclerosis Imaging
- F-18 Fluoride Positron Emission Tomography-Computed Tomography for Detecting Atherosclerotic Plaques
