Detecting Metastatic Bladder Cancer Using 18F-Fluorodeoxyglucose Positron-Emission Tomography/Computed Tomography
- Affiliations
-
- 1Department of Urology, Sifa University School of Medicine, Izmir, Turkey. drhakanozturk@yahoo.com.tr
- KMID: 2403403
- DOI: http://doi.org/10.4143/crt.2014.157
Abstract
- PURPOSE
The purpose of this study was to retrospectively investigate the contribution of 18F-fluorodeoxyglucose-positron emission tomography/computed tomography (18F-FDG-PET/CT) to detection of metastatic bladder cancer.
MATERIALS AND METHODS
The present study included 79 patients (69 men and 10 women) undergoing 18F-FDG-PET/CT upon suspicion of metastatic bladder cancer between July 2007 and April 2013. The mean age was 66.1 years with a standard deviation of 10.7 years (range, 21 to 85 years). Patients were required to fast for 6 hours prior to scanning, and whole-body PET scanning from the skull base to the upper thighs was performed approximately 1 hour after intravenous injection of 555 MBq of 18F-FDG. Whole body CT scanning was performed in the cranio-caudal direction. FDG-PET images were reconstructed using CT data for attenuation correction. Suspicious recurrent or metastatic lesions were confirmed by histopathology or clinical follow-up.
RESULTS
The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 18F-FDG-PET/CT were 89%, 78%, 90%, 75%, and 86%, respectively.
CONCLUSION
18F-FDG-PET/CT can detect metastases with high sensitivity and positive predictive values in patients with metastatic bladder carcinoma.
Keyword
MeSH Terms
Figure
-

Fig. 1. Distribution of metastases of patients. UTUC, upper tract urothelial carcinoma.

Fig. 2. (A) Coronal 18F-FDG-PET/CT scans (white arrow: right lung metastasis; SUVmax, 14.6; red arrow: false-positive FDG accumulation in the left lung, pneumonia; SUVmax, 5.0). (B) Coronal 18F-FDG-PET/CT scans (arrow: liver metastasis; SUVmax, 6.4). (C) Coronal 18F-FDG-PET/CT scans (arrow: metastatic mass filling the neural foramina at the level of L2 vertebra; SUVmax, 12.0). 18F-FDG-PET/CT, fluorodeoxyglucose-positron emission tomography/computed tomography; SUVmax, maximum standardized uptake value.
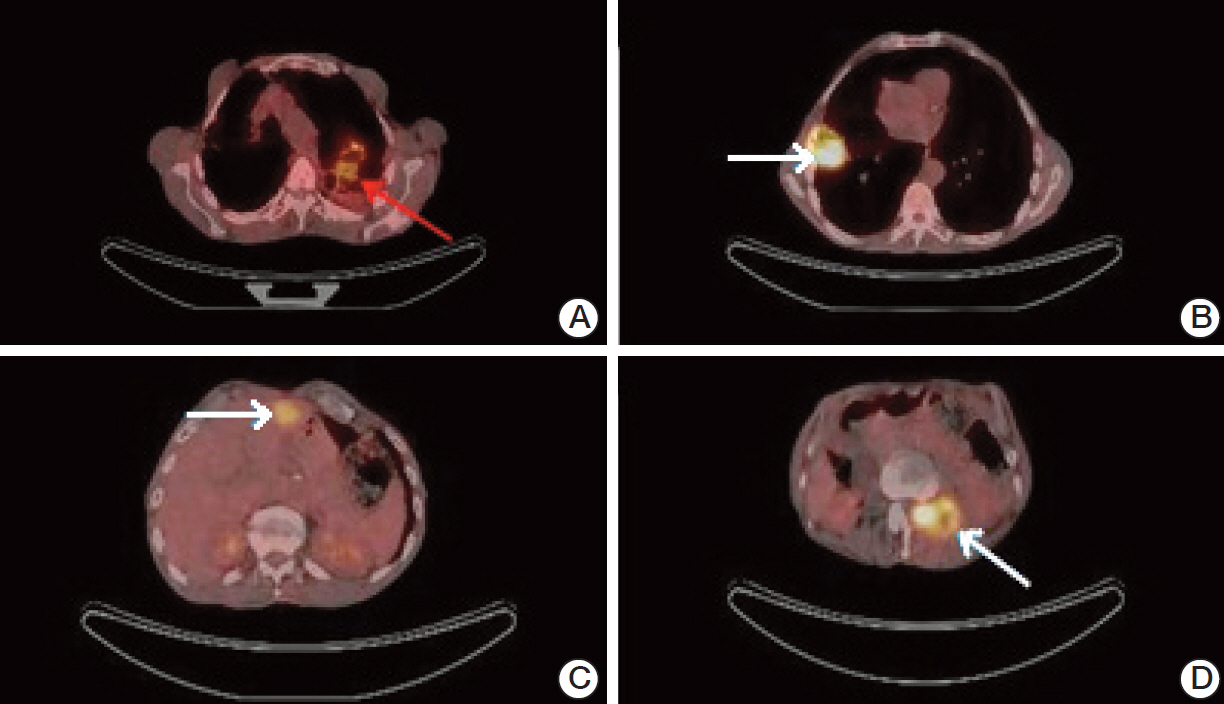
Fig. 3. (A) Axial 18F-FDG-PET/CT scans (arrow: false-positive FDG accumulation in the left lung, pneumonia; SUVmax, 5.0). (B) Axial 18F-FDG-PET/CT scans (arrow: right lung metastasis; SUVmax, 14.6). (C) Axial 18F-FDG-PET/CT scans (arrow: liver metastasis; SUVmax, 6.4). (D) Axial 18F-FDG-PET/CT scans (arrow: metastatic mass filling the neural foramina at the level of L2 vertebra; SUVmax, 12.0). 18F-FDG-PET/CT, fluorodeoxyglucose-positron emission tomography/computed tomography; SUVmax, maximum standardized uptake value.
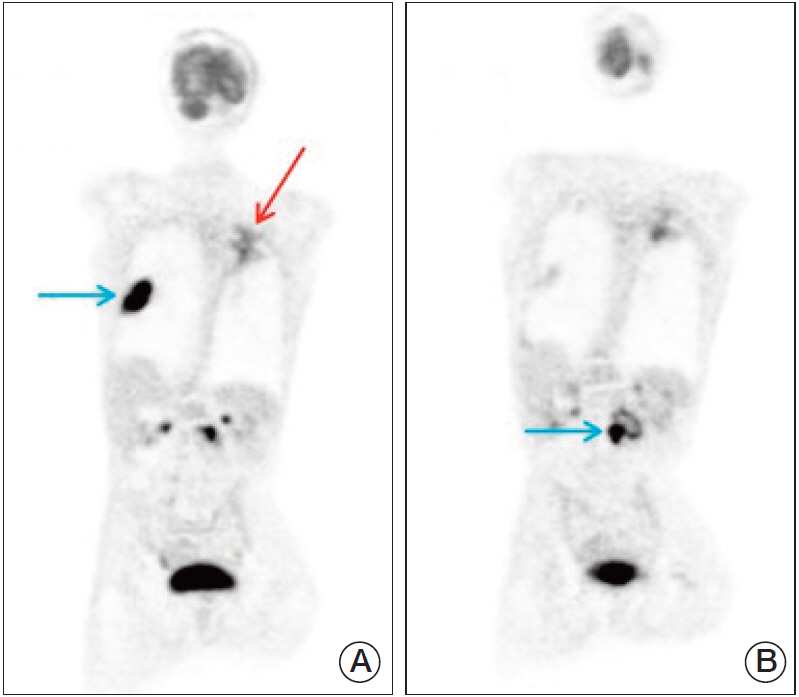
Fig. 4. (A) Maximum intensity projection (MIP) images of a patient (blue arrow: right lung metastasis; red arrow: false-positive fluorodeoxyglucose accumulation in the left lung, pneumonia). (B) MIP images of a patient (arrow: L2 vertebral metastasis).
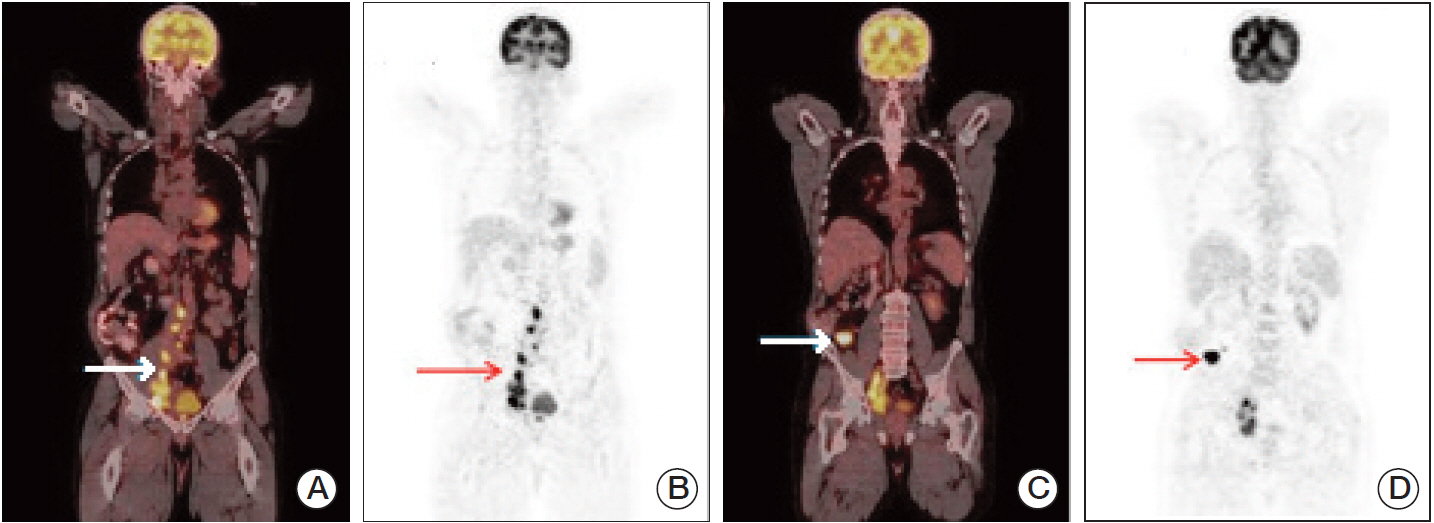
Fig. 5. (A) Coronal 18F-FDG-PET/CT scans (arrow: widespread retroperitoneal lymph node metastasis; SUVmax, 20.3). (B) MIP images of a patient (arrow: widespread retroperitoneal lymph node metastasis). (C) Coronal 18F-FDG-PET/CT scans (arrow: soft tissue metastasis; SUVmax, 18.2). (D) MIP images of a patient (arrow: soft tissue metastasis). 18F-FDG-PET/CT, fluorodeoxyglucose-positron emission tomography/computed tomography; SUVmax, maximum standardized uptake value; MIP, maximum intensity projection.
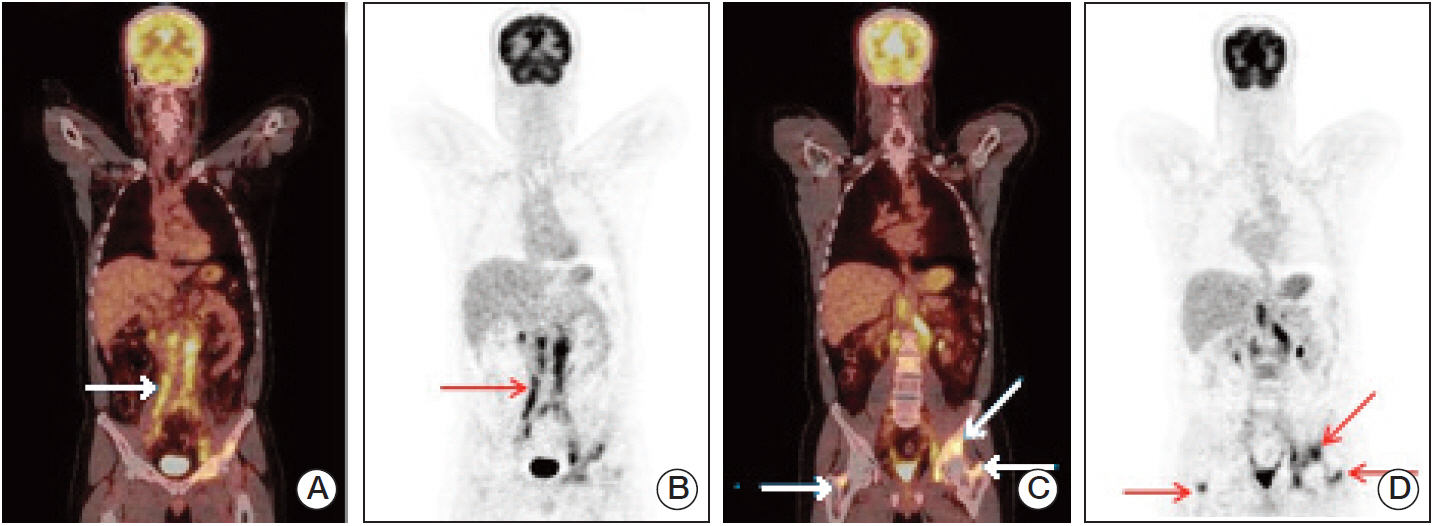
Fig. 6. (A) Coronal 18F-FDG-PET/CT scans (arrow: widespread conglomerate retroperitoneal lymph node metastasis; SUVmax, 10.8). (B) MIP images of a patient (arrow: widespread conglomerate retroperitoneal lymph node metastasis). (C) Coronal 18F-FDG-PET/CT scans (arrows: widespread bone metastasis; SUVmax, 13.5). (D) MIP images of a patient (arrows: widespread bone metastasis). 18F-FDG-PET/CT, fluorodeoxyglucose-positron emission tomography/computed tomography; SUVmax, maximum standardized uptake value; MIP, maximum intensity projection.
Reference
-
References
1. Ploeg M, Aben KK, Kiemeney LA. The present and future burden of urinary bladder cancer in the world. World J Urol. 2009; 27:289–93.
Article2. Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin. 2011; 61:212.3. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013; 63:11–30.
Article4. Abdollah F, Gandaglia G, Thuret R, Schmitges J, Tian Z, Jeldres C, et al. Incidence, survival and mortality rates of stage-specific bladder cancer in United States: a trend analysis. Cancer Epidemiol. 2013; 37:219–25.
Article5. Kaufman DS, Shipley WU, Feldman AS. Bladder cancer. Lancet. 2009; 374:239–49.
Article6. Stein JP, Lieskovsky G, Cote R, Groshen S, Feng AC, Boyd S, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol. 2001; 19:666–75.
Article7. Sternberg CN, Pansadoro V, Calabro F, Schnetzer S, Giannarelli D, Emiliozzi P, et al. Can patient selection for bladder preservation be based on response to chemotherapy? Cancer. 2003; 97:1644–52.
Article8. Barentsz JO, Engelbrecht MR, Witjes JA, de la Rosette JJ, van der Graaf M. MR imaging of the male pelvis. Eur Radiol. 1999; 9:1722–36.
Article9. Bouchelouche K, Turkbey B, Choyke PL. PET/CT and MRI in bladder cancer. J Cancer Sci Ther. 2012; S14:7692.
Article10. Jadvar H, Quan V, Henderson RW, Conti PS. [F-18]-Fluorodeoxyglucose PET and PET-CT in diagnostic imaging evaluation of locally recurrent and metastatic bladder transitional cell carcinoma. Int J Clin Oncol. 2008; 13:42–7.
Article11. Lu YY, Chen JH, Liang JA, Wang HY, Lin CC, Lin WY, et al. Clinical value of FDG PET or PET/CT in urinary bladder cancer: a systemic review and meta-analysis. Eur J Radiol. 2012; 81:2411–6.
Article12. Harney JV, Wahl RL, Liebert M, Kuhl DE, Hutchins GD, Wedemeyer G, et al. Uptake of 2-deoxy, 2-(18F) fluoro-D-glucose in bladder cancer: animal localization and initial patient positron emission tomography. J Urol. 1991; 145:279.13. Drieskens O, Oyen R, Van Poppel H, Vankan Y, Flamen P, Mortelmans L. FDG-PET for preoperative staging of bladder cancer. Eur J Nucl Med Mol Imaging. 2005; 32:1412–7.
Article14. Apolo AB, Riches J, Schoder H, Akin O, Trout A, Milowsky MI, et al. Clinical value of fluorine-18 2-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography in bladder cancer. J Clin Oncol. 2010; 28:3973–8.
Article15. Kibel AS, Dehdashti F, Katz MD, Klim AP, Grubb RL, Humphrey PA, et al. Prospective study of [18F]fluorodeoxyglucose positron emission tomography/computed tomography for staging of muscle-invasive bladder carcinoma. J Clin Oncol. 2009; 27:4314–20.16. Lin EC, Alavi A. Urologic tumors. In : Lin EC, Alavi A, editors. PET and PET/CT: a clinical guide. New York: Thieme;2009. p. 204–11.17. Anjos DA, Etchebehere EC, Ramos CD, Santos AO, Albertotti C, Camargo EE. 18F-FDG PET/CT delayed images after diuretic for restaging invasive bladder cancer. J Nucl Med. 2007; 48:764–70.18. Harkirat S, Anand S, Jacob M. Forced diuresis and dual-phase F-fluorodeoxyglucose-PET/CT scan for restaging of urinary bladder cancers. Indian J Radiol Imaging. 2010; 20:13–9.19. Swinnen G, Maes A, Pottel H, Vanneste A, Billiet I, Lesage K, et al. FDG-PET/CT for the preoperative lymph node staging of invasive bladder cancer. Eur Urol. 2010; 57:641–7.
Article20. Lodde M, Lacombe L, Friede J, Morin F, Saourine A, Fradet Y. Evaluation of fluorodeoxyglucose positron-emission tomography with computed tomography for staging of urothelial carcinoma. BJU Int. 2010; 106:658–63.
Article21. Jensen TK, Holt P, Gerke O, Riehmann M, Svolgaard B, Marcussen N, et al. Preoperative lymph-node staging of invasive urothelial bladder cancer with 18F-fluorodeoxyglucose positron emission tomography/computed axial tomography and magnetic resonance imaging: correlation with histopathology. Scand J Urol Nephrol. 2011; 45:122–8.22. Liu IJ, Lai YH, Espiritu JI, Segall GM, Srinivas S, Nino-Murcia M, et al. Evaluation of fluorodeoxyglucose positron emission tomography imaging in metastatic transitional cell carcinoma with and without prior chemotherapy. Urol Int. 2006; 77:69–75.
Article23. Mertens LS, Mir MC, Scott AM, Lee ST, Fioole-Bruining A, Vegt E, et al. 18F-fluorodeoxyglucose: positron emission tomography/computed tomography aids staging and predicts mortality in patients with muscle-invasive bladder cancer. Urology. 2014; 83:393–8.24. Golan S, Sopov V, Baniel J, Groshar D. Comparison of 11C-choline with 18F-FDG in positron emission tomography/computerized tomography for staging urothelial carcinoma: a prospective study. J Urol. 2011; 186:436–41.25. El Fakhri G, Surti S, Trott CM, Scheuermann J, Karp JS. Improvement in lesion detection with whole-body oncologic time-of-flight PET. J Nucl Med. 2011; 52:347–53.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 18F-2-Deoxy-2-Fluoro-D-Glucose Positron Emission Tomography: Computed Tomography for Preoperative Staging in Gastric Cancer Patients
- The Clinical Roles of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computerized Tomography for Urological Disease
- Supraclavicular Lymph Node Metastasis from Various Malignancies: Assessment with 18F-Fluorodeoxyglucose Positron Emission Tomography/CT, Contrast-Enhanced CT and Ultrasound
- Late Port Site Metastasis from Occult Gall Bladder Carcinoma After Laparoscopic Cholecystectomy for Cholelithiasis: The Role of 18F-FDG PET/CT
- 18F-FDG PET/CT Findings in a Breast Cancer Patient with Concomitant Tuberculous Axillary Lymphadenitis
