Importance of Individual Ghost Cells in Fine-Needle Aspiration Cytology Diagnosis of Pilomatricoma
- Affiliations
-
- 1Department of Pathology, Korea Cancer Center Hospital, Korea Institute of Radiological and Medical Sciences (KIRAMS), Seoul, Korea.
- 2Laboratory of Radiation Pathology, Korea Institute of Radiological and Medical Sciences (KIRAMS), Seoul, Korea. sslee@kirams.re.kr
- KMID: 2403257
- DOI: http://doi.org/10.4132/jptm.2017.10.18
Abstract
- BACKGROUND
Although histological diagnosis of pilomatricoma is not difficult because of its unique histological features, cytological diagnosis through fine-needle aspiration cytology (FNAC) is often problematic due to misdiagnoses as malignancy.
METHODS
We reviewed the cytological features of 14 cases of histologically-proven pilomatricoma from Korea Cancer Center Hospital, with a discussion on the diagnostic pitfalls of FNAC.
RESULTS
Among 14 cases of pilomatricoma, 10 (71.4%) were correctly diagnosed through FNAC, and two (14.3%) were misdiagnosed as carcinoma. Cytologically, all cases had easily recognizable clusters of basaloid cells and foreign body-type multinucleated cells. Although ghost cells were also found in all cases, some were inconspicuous and hardly recognizable due to their small numbers.
CONCLUSIONS
An accurate diagnosis of pilomatricoma in FNAC is feasible with consideration of clinical information and close examination of ghost cells.
Figure
-

Fig. 1. Cytological features of pilomatricoma. (A) Low power view exhibiting large clusters of basaloid cells, ghost cells (thick arrows), and a multinucleated giant cell (thin arrow) in an inflammatory background. (B) Large clusters of basaloid cells mimicking carcinoma. (C) Ghost cells. (D) Nucleated squamous cells. (E) Foreign body-type multinucleated giant cell (right upper), small cluster of basaloid cells (left upper), calcific debris (lower), isolated ghost cell (arrow), and inflammatory cells. (F) Cellular debris (Papanicolaou stain).
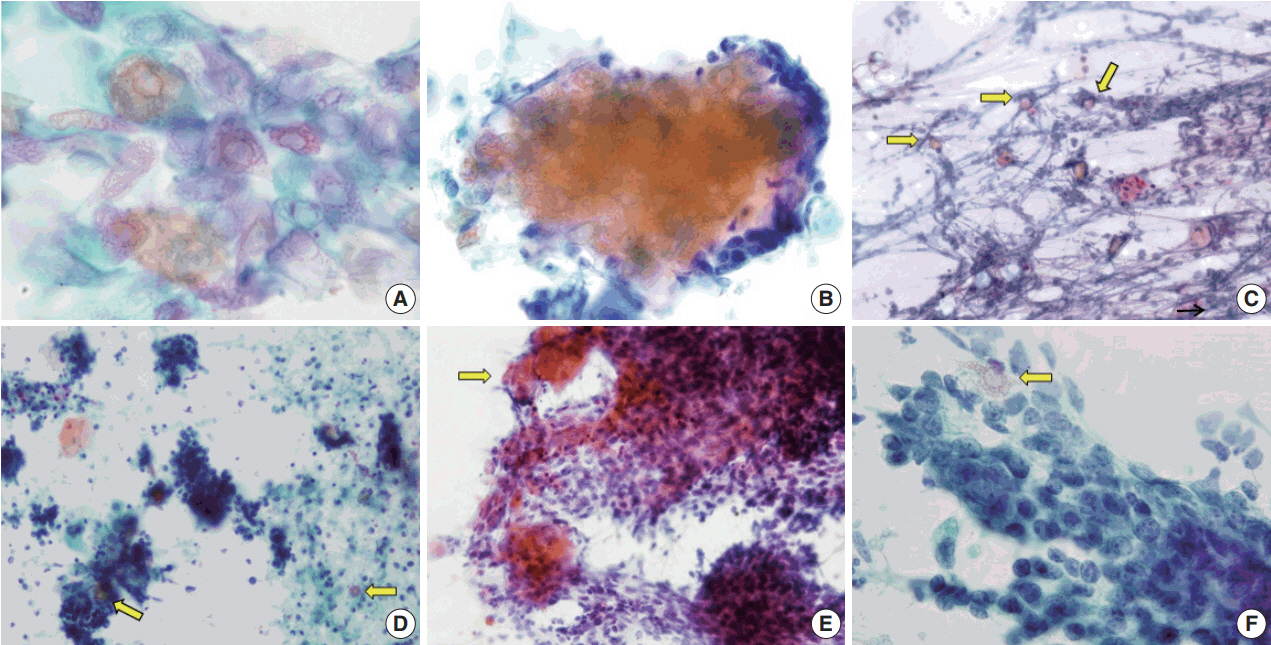
Fig. 2. Variable features of ghost cells in aspirates of pilomatricoma. (A) Ghost cell sheet showing abundant cytoplasm with distinct cell borders and central unstained area. (B) Clusters of ghost cells with peripheral basaloid cells. (C) Isolated ghost cells (arrows) and a small cluster of nucleated squamous cells in an inflammatory background. (D) Predominance of basaloid cell clusters and a few ghost cells (arrows). (E) Ghost cell nests (arrow) at the periphery of a large cluster of basaloid cells. (F) A single ghost cell (arrow) can be overlooked due to a basaloid cell cluster.
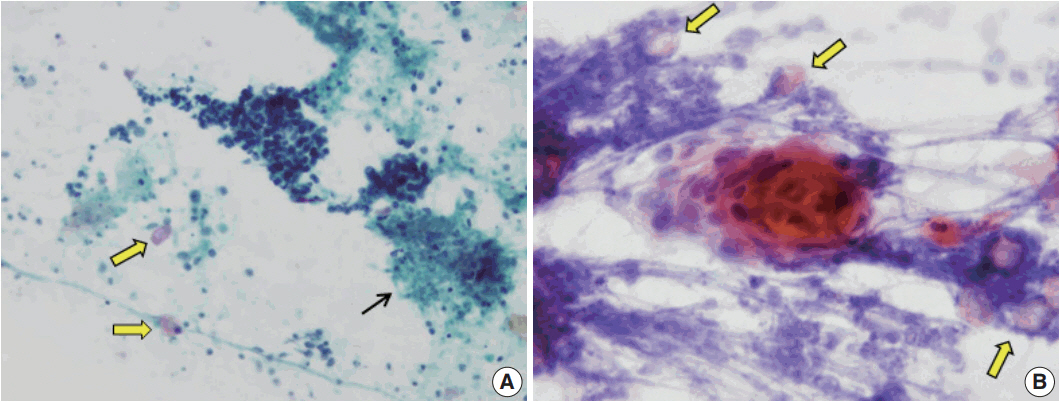
Fig. 3. Fine-needle aspiration cytology smear from pilomatricoma mimicking carcinoma. (A) Tight clusters of basaloid cells and necrotic debris (thin arrow) simulate carcinoma. However, a few scattered ghost cells are noted (thick arrows). (B) A nest of nucleated keratinizing squamous cells (center) may raise the suspicion of carcinoma. Nevertheless, if ghost cells are noted (arrows), a correct diagnosis of pilomatricoma can be made.
Reference
-
1. Fletcher CD. Diagnostic histopathology of tumors. 4th ed. Philadelphia: Elsevier Saunders;2013. p. 1707.2. LeBoit PE, Burg G, Weeden D, Sarasain A. World Health Organization classification of tumours: pathology and genetics of skin tumours. Lyon: IARC Press;2006. p. 153–5.3. Domanski HA, Domanski AM. Cytology of pilomatrixoma (calcifying epithelioma of Malherbe) in fine needle aspirates. Acta Cytol. 1997; 41:771–7.
Article4. Agrawal L, Kaur P, Singh J, Singh N. Pilomatrixoma misdiagnosed as round cell tumor on fine-needle aspiration cytology. Indian J Cancer. 2010; 47:483–5.
Article5. Sharma D, Agarwal S, Jain LS, Kamal V. Pilomatrixoma masquerading as metastatic adenocarcinoma: a diagnostic pitfall on cytology. J Clin Diagn Res. 2014; 8:FD13–4.
Article6. Singh S, Gupta R, Mandal AK. Pilomatrixoma: a potential diagnostic pitfall in aspiration cytology. Cytopathology. 2007; 18:260–2.
Article7. Wang J, Cobb CJ, Martin SE, Venegas R, Wu N, Greaves TS. Pilomatrixoma: clinicopathologic study of 51 cases with emphasis on cytologic features. Diagn Cytopathol. 2002; 27:167–72.
Article8. Bhatt MK, Sommerville R, Ravi Kumar AS. FDG PET/CT appearance of benign pilomatricoma. Clin Nucl Med. 2012; 37:684–6.
Article9. Tay JK, Nga ME, Loh KS. Pilomatricoma of the cheek: a benign tumor mimicking metastatic squamous cell carcinoma on FDG PET/CT. Am J Otolaryngol. 2014; 35:452–5.
Article10. Szturz P, Rehák Z, Koukalová R, Adam Z, Mayer J. FDG-PET positive pilomatrixoma: reconsidering multicentricity in Langerhans cell histiocytosis. Nucl Med Rev Cent East Eur. 2014; 17:94–6.11. Jung YS, Kang JG, Park WS, Ryu J. Pilomatricoma: diagnostic pitfalls in PET/CT and fine-needle aspiration biopsy. Otolaryngol Head Neck Surg. 2007; 137:845–6.
Article12. Pirouzmanesh A, Reinisch JF, Gonzalez-Gomez I, Smith EM, Meara JG. Pilomatrixoma: a review of 346 cases. Plast Reconstr Surg. 2003; 112:1784–9.13. Rosenbaum SJ, Lind T, Antoch G, Bockisch A. False-positive FDG PET uptake: the role of PET/CT. Eur Radiol. 2006; 16:1054–65.14. Lan MY, Lan MC, Ho CY, Li WY, Lin CZ. Pilomatricoma of the head and neck: a retrospective review of 179 cases. Arch Otolaryngol Head Neck Surg. 2003; 129:1327–30.15. Cigliano B, Baltogiannis N, De Marco M, et al. Pilomatricoma in childhood: a retrospective study from three European paediatric centres. Eur J Pediatr. 2005; 164:673–7.
Article16. Al-Khateeb TH, Hamasha AA. Pilomatricoma of the maxillofacial area in the northern regional Jordanian population: report of 31 cases. J Oral Maxillofac Surg. 2007; 65:261–6.
Article17. Gupta M, Bansal R, Tiwari G, Sharma S. Aggressive pilomatrixoma: a diagnostic dilemma on fine-needle aspiration cytology with review of literature. Diagn Cytopathol. 2014; 42:906–11.18. Ieni A, Todaro P, Bonanno AM, Catalano F, Catalano A, Tuccari G. Limits of fine-needle aspiration cytology in diagnosing pilomatrixoma: a series of 25 cases with clinico-pathologic correlations. Indian J Dermatol. 2012; 57:152–5.
Article19. Lemos MM, Kindblom LG, Meis-Kindblom JM, Ryd W, Willén H. Fine-needle aspiration features of pilomatrixoma. Cancer. 2001; 93:252–6.
Article20. Nori J, Abdulcadir D, Giannotti E, Calabrese M. Pilomatrixoma of the breast, a rare lesion simulating breast cancer: a case report. J Radiol Case Rep. 2013; 7:43–50.
Article21. Bansal C, Handa U, Mohan H. Fine needle aspiration cytology of pilomatrixoma. J Cytol. 2011; 28:1–6.
Article22. Kumaran N, Azmy A, Carachi R, Raine PA, Macfarlane JH, Howatson AG. Pilomatrixoma--accuracy of clinical diagnosis. J Pediatr Surg. 2006; 41:1755–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fine Needle Aspiration Cytology of a Pilomatrixoma Misdiagnosed as Carcinoma: A Case Report
- Diagnostic Pitfalls in Breast Fine Needle Aspiration Cytology: False Positive and False Negative
- Fine Needle Aspiration Cytology of Thyroid Follicular Proliferative Lesions
- Fine Needle Aspiration Cytology of Mucoepidermoid Carcinoma of the Lung: A Case Report
- Fine Needle Aspiration Cytology of Langerhans' Cell Histiocytosis in the Lymph Node
