Korean Circ J.
2018 Feb;48(2):148-158. 10.4070/kcj.2017.0179.
The Complexity of Pediatric Multifocal Atrial Tachycardia and Its Prognostic Factors
- Affiliations
-
- 1Department of Pediatrics, Seoul National University Children's Hospital, Seoul, Korea. mksong52@gmail.com
- KMID: 2403162
- DOI: http://doi.org/10.4070/kcj.2017.0179
Abstract
- BACKGROUND AND OBJECTIVES
Multifocal atrial tachycardia (MAT), in general, has a favorable outcome. However, there are insufficient data regarding MAT in a pediatric population. This study sought to determine the clinical course of MAT and identify potential prognostic factors.
METHODS
The medical records of MAT patients from 1997-2015 were reviewed. The arrhythmia control rate and factors for unfavorable outcomes were assessed and compared to those in the literature.
RESULTS
Of the 33 included patients (19 boys and 14 girls), 27 were infants less than 1 year of age. The median age at diagnosis was 1.7 months (range, 0 day to 14 years). Fourteen (42%) patients had structural heart disease. Eight (24%) patients had lung disease and 6 (18%) had a syndromic diagnosis belonging to RASopathy. Two patients developed polymorphic ventricular tachycardia, in whom genetic analysis confirmed the presence of the RyR2 mutation several years later. MAT was controlled in 26 patients (84%) within 3.9 months (median; range, 16 days-18.4 years) using an average of 2.4 medications. There were 3 cases of cardiopulmonary mortality. The arrhythmia control rate was higher in the infant group (85%) than in the non-infant group (67%), although this trend was not statistically significant. There was a significantly lower rate of unfavorable outcomes in the idiopathic infant group (n=11) than in the other groups (p=0.008). Considering the findings of previous studies, the mortality rate was significantly higher in patients with structural heart disease than in patients without (21% vs. 5%, p=0.01).
CONCLUSIONS
MAT usually affects infants and has a favorable prognosis, particularly in the idiopathic infant group. However, in the presence of other comorbidities, MAT may have a variable clinical course.
MeSH Terms
Figure
-
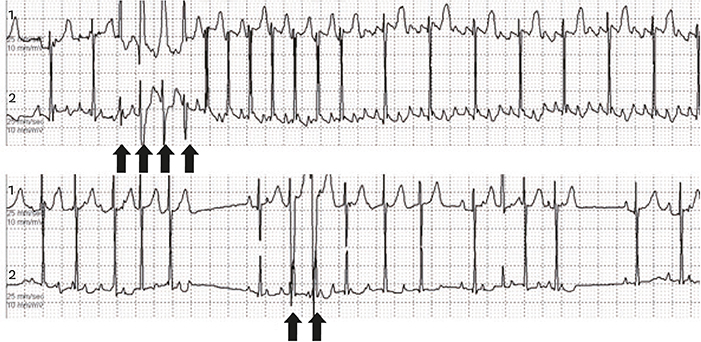
Figure 1 Holter monitoring of multifocal atrial tachycardia showed irregular narrow-QRS tachycardia with aberrantly conducted wide QRS complexes (arrows) and multiple morphologically distinct P-waves with variable P-R intervals.
Cited by 1 articles
-
Clinical Implication of Multifocal Atrial Tachycardia in Children for Pediatric Cardiologist
June Huh
Korean Circ J. 2018;48(2):173-175. doi: 10.4070/kcj.2018.0037.
Reference
-
1. Bradley DJ, Fischbach PS, Law IH, Serwer GA, Dick M 2nd. The clinical course of multifocal atrial tachycardia in infants and children. J Am Coll Cardiol. 2001; 38:401–408.
Article2. Lazaros G, Chrysohoou C, Oikonomou E, et al. The natural history of multifocal atrial rhythms in elderly outpatients: insights from the “Ikaria study”. Ann Noninvasive Electrocardiol. 2014; 19:483–489.
Article3. Kastor JA. Multifocal atrial tachycardia. N Engl J Med. 1990; 322:1713–1717.
Article4. Fish FA, Mehta AV, Johns JA. Characteristics and management of chaotic atrial tachycardia of infancy. Am J Cardiol. 1996; 78:1052–1055.5. Liberthson RR, Colan SD. Multifocal or chaotic atrial rhythm: report of nine infants, delineation of clinical course and management, and review of the literature. Pediatr Cardiol. 1982; 2:179–184.6. Yeager SB, Hougen TJ, Levy AM. Sudden death in infants with chaotic atrial rhythm. Am J Dis Child. 1984; 138:689–692.
Article7. Dodo H, Gow RM, Hamilton RM, Freedom RM. Chaotic atrial rhythm in children. Am Heart J. 1995; 129:990–995.
Article8. Salim MA, Case CL, Gillette PC. Chaotic atrial tachycardia in children. Am Heart J. 1995; 129:831–833.
Article9. Farooki ZQ, Green EW. Multifocal atrial tachycardia in two neonates. Br Heart J. 1977; 39:872–874.
Article10. Beitzke A. Multifocal (chaotic) atrial tachycardia in infancy. Helv Paediatr Acta. 1979; 34:319–327.11. Chantepie A, Ramponi N, Vaillant MC, Laugier J, Raynaud P, Fauchier JP. Polymorphic atrial tachycardia and Wolff-Parkinson-White syndrome in a newborn infant. Arch Mal Coeur Vaiss. 1986; 79:1371–1375.12. Bisset GS 3rd, Seigel SF, Gaum WE, Kaplan S. Chaotic atrial tachycardia in childhood. Am Heart J. 1981; 101:268–272.
Article13. Lipson MJ, Naimi S. Multifocal atrial tachycardia (chaotic atrial tachycardia). Clinical associations and significance. Circulation. 1970; 42:397–407.14. Tutar E, Çiftçi Ö, Fitoz S, et al. Lipomatous hypertrophy of the interatrial septum in a child with atrial tachycardia. Pediatr Int. 2016; 58:523–525.
Article15. Hsieh MY, Lee PC, Hwang B, Meng CC. Multifocal atrial tachycardia in 2 children. J Chin Med Assoc. 2006; 69:439–443.
Article16. Di Pino A, Caruso E, Costanzo L, Guccione P. A novel RyR2 mutation in a 2-year-old baby presenting with atrial fibrillation, atrial flutter, and atrial ectopic tachycardia. Heart Rhythm. 2014; 11:1480–1483.
Article17. Broendberg AK, Nielsen JC, Bjerre J, et al. Nationwide experience of catecholaminergic polymorphic ventricular tachycardia caused by RyR2 mutations. Heart. 2017; 103:901–909.
Article18. Lin AE, Alexander ME, Colan SD, et al. Clinical, pathological, and molecular analyses of cardiovascular abnormalities in Costello syndrome: a Ras/MAPK pathway syndrome. Am J Med Genet A. 2011; 155A:486–507.
Article19. Prada CE, Zarate YA, Hagenbuch S, Lovell A, Schorry EK, Hopkin RJ. Lethal presentation of neurofibromatosis and Noonan syndrome. Am J Med Genet A. 2011; 155A:1360–1366.
Article20. Finsterer J, Stollberger C, Stubenberger E, Tschakoschian S. Lymphangiopathy in neurofibromatosis 1 manifesting with chylothorax, pericardial effusion, and leg edema. Int J Gen Med. 2013; 6:743–746.
Article21. Pickoff AS, Singh S, Flinn CJ, McCormack J, Stolfi A, Gelband H. Atrial vulnerability in the immature canine heart. Am J Cardiol. 1985; 55:1402–1406.
Article22. Zeevi B, Berant M, Sclarovsky S, Blieden LC. Treatment of multifocal atrial tachycardia with amiodarone in a child with congenital heart disease. Am J Cardiol. 1986; 57:344–345.
Article23. Houyel L, Fournier A, Davignon A. Successful treatment of chaotic atrial tachycardia with oral flecainide. Int J Cardiol. 1990; 27:27–29.
Article24. Cetta F, Bell TJ, Ros SP. Emergency department evaluation of an infant with chaotic atrial tachycardia. Pediatr Emerg Care. 1997; 13:120–122.
Article25. Bouziri A, Khaldi A, Hamdi A, et al. Multifocal atrial tachycardia: an unusual cause of cardiogenic shock in a newborn. Tunis Med. 2011; 89:59–61.26. Pregowska K, Jurkiewicz E, Miszczak-Knecht M, Turska-Kmiec A, Bieganowska K. Persistent multifocal atrial tachycardia in infant with encephalocraniocutaneous lipomatosis: a case report. Eur J Pediatr. 2014; 173:1577–1580.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Implication of Multifocal Atrial Tachycardia in Children for Pediatric Cardiologist
- Multifocal Atrial Tachycardia in a Newborn
- Immediate Improvement of Chaotic Atrial Tachycardia after Ligation of Patent Ductus Arteriosus
- Differential Diagnosis of Supraventricular Tachycardia
- Atrial Fibrillation with Ventricular Pre-excitation after Intravenous Adenosine as a Treatment of Supraventricular Tachycardia
