Ann Surg Treat Res.
2018 Feb;94(2):83-87. 10.4174/astr.2018.94.2.83.
A novel robotic right colectomy for colon cancer via the suprapubic approach using the da Vinci Xi system: initial clinical experience
- Affiliations
-
- 1Colorectal Cancer Center, Kyungpook National University Medical Center, Kyungpook National University School of Medicine, Daegu, Korea. kyuschoi@mail.knu.ac.kr
- KMID: 2402850
- DOI: http://doi.org/10.4174/astr.2018.94.2.83
Abstract
- PURPOSE
We developed a technique of totally-robotic right colectomy with D3 lymphadenectomy and intracorporeal anastomosis via a suprapubic transverse linear port. This article aimed to introduce our novel robotic surgical technique and assess the short-term outcomes in a series of five patients.
METHODS
All colectomies were performed using the da Vinci Xi system. Four robot trocars were placed transversely in the supra pubic area. Totally-robotic right colectomy was performed, including colonic mobilization, D3 lymphadenectomy, and intra corporeal stapled functional anastomosis. The 2 middle suprapubic trocar incisions were then extended to retrieve the specimen.
RESULTS
Five robotic right colectomies via the suprapubic approach were performed between August 2015 and February 2016. The mean operation time was 183 ± 29.37 minutes, and the mean estimated blood loss was 27 ± 9.75 mL. The time to clear liquid intake was 3 days in all patients, and the mean length of stay after surgery was 6.2 ± 0.55 days. No patient required conversion to conventional laparoscopic surgery. There were no perioperative complications. According to the pathology report, the mean number of harvested lymph nodes was 36.6 ± 4.45. Four patients were stage III, and 1 patient was stage II according to the 7th edition of the American Joint Committee on Cancer system.
CONCLUSION
Totally-robotic right colectomy via the suprapubic approach can be performed successfully in selected patients. Further comparative studies are required to verify the clinical advantages of our technique over conventional robotic surgery.
MeSH Terms
Figure
-
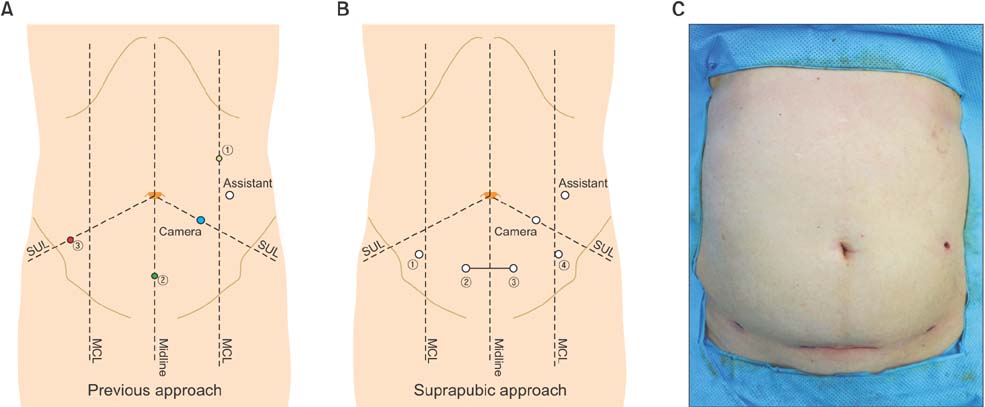
Fig. 1 Suprapubic approach. (A) Trocar positioning of da Vinci Si system. (B) Novel trocar positioning of da Vinci Xi system. (C) A postoperative scar after suprapubic approach. SUL, spinoumbilicus line; MCL, midclavicular line.
Cited by 1 articles
-
Robotic surgery for colorectal disease: review of current port placement and future perspectives
Jong Lyul Lee, Hassan A. Alsaleem, Jin Cheon Kim
Ann Surg Treat Res. 2020;98(1):31-43. doi: 10.4174/astr.2020.98.1.31.
Reference
-
1. Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet. 2002; 359:2224–2229.
Article2. Clinical Outcomes of Surgical Therapy Study Group. Nelson H, Sargent DJ, Wieand HS, Fleshman J, Anvari M, et al. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004; 350:2050–2059.
Article3. Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, Beart RW Jr, et al. Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg. 2007; 246:655–662.
Article4. Park JS, Choi GS, Lim KH, Jang YS, Jun SH. Robotic-assisted versus laparoscopic surgery for low rectal cancer: case-matched analysis of short-term outcomes. Ann Surg Oncol. 2010; 17:3195–3202.
Article5. Xu H, Li J, Sun Y, Li Z, Zhen Y, Wang B, et al. Robotic versus laparoscopic right colectomy: a meta-analysis. World J Surg Oncol. 2014; 12:274.
Article6. Trastulli S, Coratti A, Guarino S, Piagnerelli R, Annecchiarico M, Coratti F, et al. Robotic right colectomy with intracorporeal anastomosis compared with laparoscopic right colectomy with extracorporeal and intracorporeal anastomosis: a retrospective multicentre study. Surg Endosc. 2015; 29:1512–1521.
Article7. Park JS, Choi GS, Park SY, Kim HJ, Ryuk JP. Randomized clinical trial of robot-assisted versus standard laparoscopic right colectomy. Br J Surg. 2012; 99:1219–1226.
Article8. Park SY, Choi GS, Park JS, Kim HJ, Choi WH, Ryuk JP. Robot-assisted right colectomy with lymphadenectomy and intracorporeal anastomosis for colon cancer: technical considerations. Surg Laparosc Endosc Percutan Tech. 2012; 22:e271–e276.9. Ozben V, Cengiz TB, Atasoy D, Bayraktar O, Aghayeva A, Erguner I, et al. Is da Vinci Xi better than da Vinci Si in robotic rectal cancer surgery? Comparison of the 2 generations of da Vinci Systems. Surg Laparosc Endosc Percutan Tech. 2016; 26:417–423.
Article10. Corcione F, Esposito C, Cuccurullo D, Settembre A, Miranda N, Amato F, et al. Advantages and limits of robot-assisted laparoscopic surgery: preliminary experience. Surg Endosc. 2005; 19:117–119.
Article11. Delaney CP, Lynch AC, Senagore AJ, Fazio VW. Comparison of robotically performed and traditional laparoscopic colorectal surgery. Dis Colon Rectum. 2003; 46:1633–1639.
Article12. Fanning J, Pruett A, Flora RF. Feasibility of the Maylard transverse incision for ovarian cancer cytoreductive surgery. J Minim Invasive Gynecol. 2007; 14:352–355.
Article13. Levrant SG, Bieber E, Barnes R. Risk of anterior abdominal wall adhesions increases with number and type of previous laparotomy. J Am Assoc Gynecol Laparosc. 1994; 1(4, Part 2):S19.
Article14. Manusook S, Suwannarurk K, Pongrojpaw D, Bhamarapravatana K. Maylard incision in gynecologic surgery: 4-year experience in Thammasat University Hospital. J Med Assoc Thai. 2014; 97:Suppl 8. S102–S107.15. Benlice C, Stocchi L, Costedio MM, Gorgun E, Kessler H. Impact of the specific extraction-site location on the risk of in ci sional hernia after laparoscopic colorectal resection. Dis Colon Rectum. 2016; 59:743–750.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The da Vinci Xi System in Robotic Gastric Cancer Surgery: A Comparison with the S System
- Robotic surgery for colorectal disease: review of current port placement and future perspectives
- Robot-assisted laparoendoscopic single-site upper urinary tract surgery with da Vinci Xi surgical system: Initial experience
- Robotic Colorectal Surgery
- Initial Experience of BABA Robotic Thyroidectomy Using the Da Vinci Xi System in Incheon, Korea
