J Korean Soc Spine Surg.
2017 Sep;24(3):190-197. 10.4184/jkss.2017.24.3.190.
Analysis of Factors Affecting Postoperative Loss of Reduction in Unstable Thoracolumbar Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, College of Medicine, Soonchunhyang University Cheonan Hospital, Korea. chhong@schmc.ac.kr
- 2Department of Orthopedic Surgery, Spine Center, College of Medicine, Soonchunhyang University Hospital, Seoul, Korea.
- KMID: 2402833
- DOI: http://doi.org/10.4184/jkss.2017.24.3.190
Abstract
- STUDY DESIGN: Retrospective analysis
OBJECTIVES
Loss of fracture reduction after posterior surgery to treat unstable thoracolumbar fractures can cause several complications. We analyzed the factors influencing postoperative loss of reduction. SUMMARY OF LITERATURE REVIEW: Controversy exists about the factors causing postoperative loss of reduction in thoracolumbar fractures during the follow-up period.
MATERIALS AND METHODS
We analyzed the records of 59 patients who underwent posterior surgery for thoracolumbar unstable fractures and had completed a minimum follow-up of 1 year. Postoperative loss of reduction was defined as 30% or more loss of vertebral body height or 15° or more progression of the kyphotic angle at the 1-year follow-up compared to immediately after surgery. The associations between the patients??gender, age, level of fracture, injury of the posterior column, initial loss of fractured vertebral body height, load-sharing score, Thoraco-Lumbar Injury Classification and Severity score, number of fixed segments, type of pedicle screws, degree of postoperative reduction, degree of postoperative corrected kyphotic angle, changes in the insertion angle of the most proximal and the most distal pedicle screws, decreases in the upper and lower disc height of the fractured vertebral body, and postoperative loss of reduction were analyzed.
RESULTS
Thirteen patients (22.0%) had postoperative loss of reduction. Age at the time of the operation (p=0.034), initial loss of fractured vertebral body height (p=0.042), and changes in the insertion angles of the most distal pedicle screws (p=0.021) were significantly associated with postoperative loss of reduction. However, the other factors did not show a significant relationship.
CONCLUSIONS
In patients who underwent posterior surgery for unstable thoracolumbar fractures, the frequency of loss of reduction was high in patients more than 45 years old at the time of the operation, with a 50% or more loss of the initial fractured vertebral body height, and with changes of 5° or more in the insertion angles of the most distal pedicle screws.
Figure
-
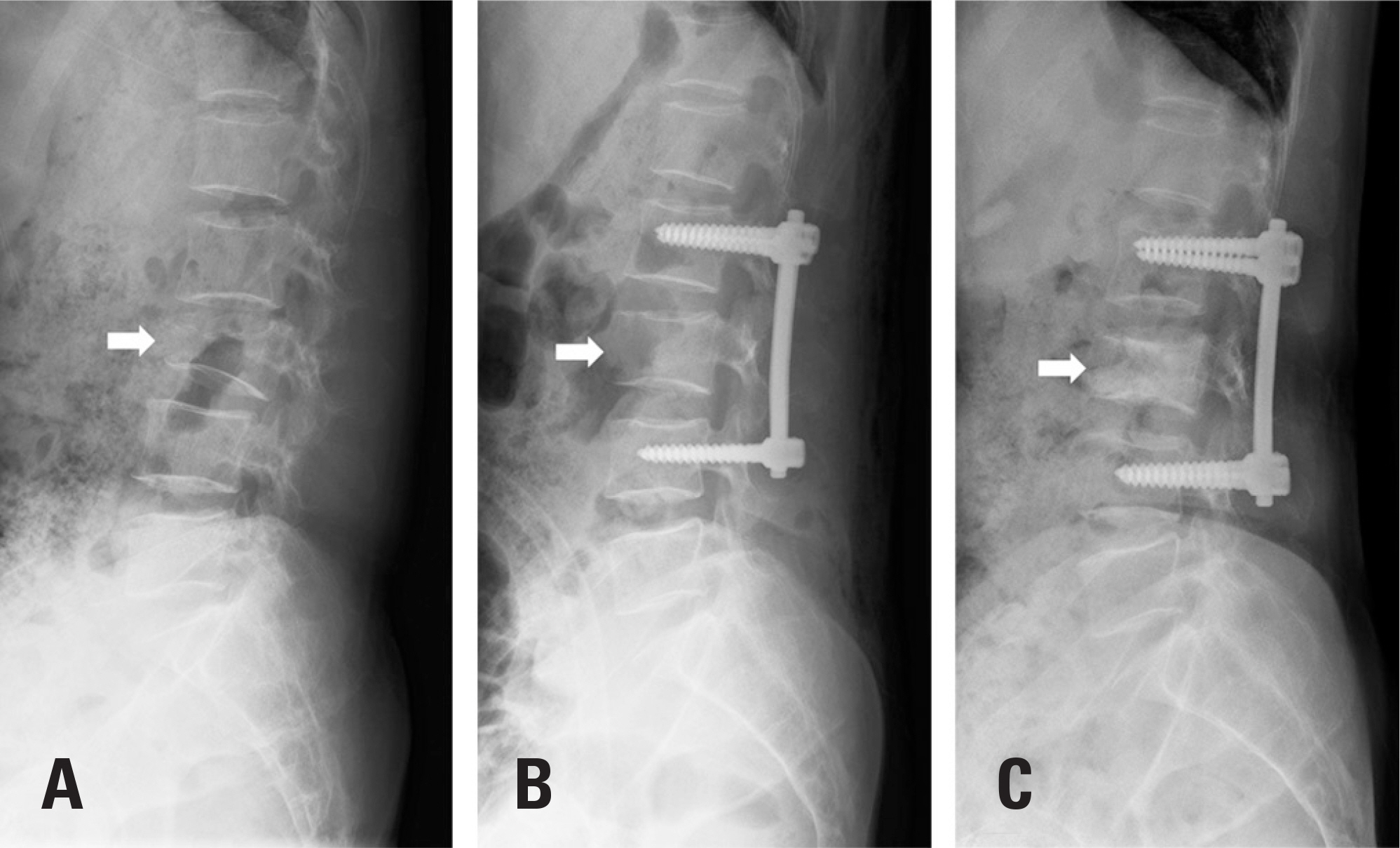
Fig. 1. Three simple plane lateral radiographs show that (A) the loss of the preoperative fracture vertebral body height was 50% or more at the L3 level, (B) postoperative reduction of the L3 body height was nearly normal, and (C) postoperative loss of reduction at the 1-year follow-up was 30% or more.
Reference
-
1. Denis F. Three column spine and its significanca in the classification of acute thoracolumbar spinal injuries. Spine (Phila Pa 1976). 1983; 8:817–31.2. McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spine fractures. Spine (Phila Pa 1976). 1994; 19:1741–4.
Article3. Vaccaro AR, Zeiller SC, Hulbert RJ, et al. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005; 18:209–15.4. Mahar A, Kim C, Wedemeyer M, et al. Short-segment fixation of lumbar burst fractures using pedicle fixation at the level of the fracture. Spine (Phila Pa 1976). 2007; 32:1503–7.
Article5. Sjostrom L, Jacobsson O, Karlstrom G, et al. CT analysis of pedicles and screw tracts after implant removal in thoracolumbar fractures. J Spinal Disord. 1993; 6:225–31.6. Yue JJ, Sossan A, Selgrath C, et al. The treatment of unstable thoracic spine fractures with transpedicular screw instrumentation: a 3-year consecutive series. Spine (Phila Pa 1976). 2002; 27:2782–7.7. Carl AL, Tromanhauser SG, Roger DJ. Pedicle screw instrumentation for thoracolumbar burst fractures and fracture-dislocations. Spine (Phila Pa 1976). 1992; 17(Suppl):317–24.
Article8. Dickson JH, Harrington PR, Erwin WD. Results of reduction and stabilization of the severely fractured thoracic and lumbar spine. J Bone Joint Surg Am. 1978; 60:799–805.
Article9. Stambough JL. Cotrel-Dubousset instrumentation and thoracolumbar spine trauma: a review of 55 cases. J Spinal Disorders. 1994; 7:461–9.10. Stambough JL. Posterior instrumentation for thoracolumbar trauma. Clin Orthop Relat Res. 1997; 335:73–88.
Article11. Kim CH, Hwang JK, Choi YJ, et al. Treatment of thoracolumbar bursting fractures according to load-sharing classification. J Korean Fract Soc. 2005; 18:69–75.
Article12. Chen JX, Xu DL, Sheng SR, et al. Risk factors of kyphosis recurrence after implant removal in thoracolumbar burst fractures following posterior short-segment fixation. Int Orthop. 2016; 40:1253–60.
Article13. Kim GW, Jang JW, Hur H, et al. Predictive factors for a kyphosis recurrence following short-segment pedicle screw fixation including fractured vertebral body in unstable thoracolumbar burst fractures. J Korean Neurosurg Soc. 2014; 56:230–6.
Article14. Denis F, Armstrong GW, Searls K, et al. Acute thoracolumbar burst fractures in the absence of neurologic deficit. A comparison between operative and nonoperative treatment. Clin Orthop Relat Res. 1984; 189:142–9.
Article15. Holdsworth F. Fractures, dislocations, and fracture-dislocations of the spine. J Bone Joint Surg Am. 1970; 52:1534–51.
Article16. Nagel DA, Koogle TA, Piziali RL, et al. Stability of the upper lumbar spine following progressive disruptions and the application of individual internal and external fixation devices. J Bone Joint Surg Am. 1981; 63:62–70.
Article17. James KS, Wenger KH, Schlegel JD, et al. Biomechanical evaluation of the stability of thoracolumbar burst fractures. Spine (Phila Pa 1976). 1994; 19:1731–40.
Article18. Gurr KR, McAfee PC, Shih CM. Biomechanical analysis of anterior and posterior instrumentation systems after corpectomy. A calf-spine model. J Bone Joint Surg Am. 1988; 70:1182–91.
Article19. Lee KY, Sohn SK, Kim CH, et al. Posterior short-segment instrumentation of thoracic and lumbar bursting fractures - Retrospective study. J Korean Soc Spine Surg. 2001; 8:497–503.20. Gurr KR, McAfee PC. Cotrel-Dubousset instrumentation in adults. A preliminary report. Spine (Phila Pa 1976). 1988; 13:510–20.21. Alvine GF, Swain JM, Asher MA, et al. Treatment of thoracolumbar burst fractures with variable screw placement or Isola instrumentation and arthrodesis: case series and literature review. J Spinal Disord Tech. 2004; 17:251–64.22. Wagar M, Van-Popta D, Barone DG, et al. Short versus long-segment posterior fixation in the treatment of thoracolumbar junction fractures: a comparison of outcomes. Br J Neurosurg. 2017; 31:54–7.23. Wang H, Li C, Liu T, et al. Biomechanical efficacy of monoaxial or polyaxial pedicle screw and additional screw insertion at the level of fracture, in lumbar burst fracture: An experimental study. Indian J Orthop. 2012; 46:395–401.
Article24. Shin BJ, Lee JC, Kim YI, et al. More than 5 year follow-up of thoracolumbar fractures treated by pedicle screw fixation. J Korean Soc Spine Surg. 2009; 16:251–8.
Article25. Mclain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg Am. 1993; 75:162–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Assessment of Operative Reduction in Thoracolumbar and Lumbar Spine Fractures
- Operative Treatment of Dorsolumbar Fractures and Fracture Dilocations: Clinical Experiences
- The Analysis of Prognostic Factors on Unstable Burst Fracture on the Thoracolumbar Spine
- Management of Unstable Fractures and Fracture - Dislocations of the Thoracolumbar Spine with Harrington Instrumentation and Posterior Spinal Fusion
- Treatment of the Unstable Thoracolumbar Fractures Using Cotrel - Dubousset Instrumentation
