Comparison of Effects and Complications between Conventional Trabeculectomy and Trabeculectomy with a Collagen Matrix Insertion
- Affiliations
-
- 1Department of Ophthalmology, Chungnam National University Hospital, Daejeon, Korea. kkn9901700@hanmail.net
- 2Department of Ophthalmology, Chungnam National University School of Medicine, Daejeon, Korea.
- KMID: 2401678
- DOI: http://doi.org/10.3341/jkos.2018.59.1.50
Abstract
- PURPOSE
To compare the surgical outcomes between trabeculectomy with a collagen matrix (Ologen®) insertion and conventional trabeculectomy.
METHODS
An ophthalmic examination, including tonometry and a slit lamp examination, was performed 1 week, 2 weeks, 1 month, 2 months, 4 months, 6 months, and 12 months postoperatively in glaucoma patients who underwent a trabeculectomy using Ologen® (experimental group) or a conventional trabeculectomy (control group). Clinical features including success rate and complications were compared between the two groups.
RESULTS
In 21 eyes of the experimental group and 42 eyes of the control group, the success rates were 76% and 69%, respectively (p = 0.554). Needling with subconjunctival 5-fluorouracil injection or laser suture lysis of the scleral flap was required in three eyes (14.3%) in the experimental group and 18 eyes (42.9%) in the control group (p = 0.023). The types of complications differed, although the total number of complications did not differ between the two groups (23.8% vs. 19.0%, respectively; p = 0.745). The most common complication in the experimental group was an encapsulated bleb, which occurred in three eyes (14.3%), whereas an avascular bleb occurred in three eyes (7.1%) in the control group.
CONCLUSIONS
The success rate of trabeculectomy with Ologen® was comparable to that of conventional trabeculectomy. However, postoperative interventions were less commonly required after trabeculectomy with Ologen®, and the complications differed between the groups. When choosing the surgical method and examining the postoperative condition, these differences should be considered.
Keyword
MeSH Terms
Figure
-

Figure 1. Trabeculectomy of the Ologen® insertion group. (A) After a half thickness scleral flap was sutured in place. (B) Ologen® was simply positioned on the scleral flap without an anchoring suture. (C) A conjunctival suture was performed. The yellow dotted line is the boundary of the inserted Ologen®.

Figure 2. Postoperative mean intraocular pressure (IOP; with standard error bars) of the trabeculectomy with Ologen® insertion group and the conventional trabeculectomy group. The IOPs were measured at 1 week, 2 weeks, 1 month, 2 months, 4 months, 6 months, and 12 months. Although the IOP in the conventional trabeculectomy group was higher than that in the trabeculectomy with Ologen® insertion group at all of the postoperative time points, the p-value for difference was only significant at postoperative 2 weeks, 4 months, and 6 months (Mann-Whitney U test, * p < 0.05).

Figure 3. The number of mean intraocular pressure (IOP)-lowering medications (with standard error bars) for the trabeculectomy with Ologen® insertion and conventional trabeculectomy groups. The postoperative time points were at 1 week, 2 weeks, 1 month, 2 months, 4 months, 6 months, and 12 months. There was no significant difference between the two groups at any postoperative time point (Mann-Whitney U test, p > 0.05).
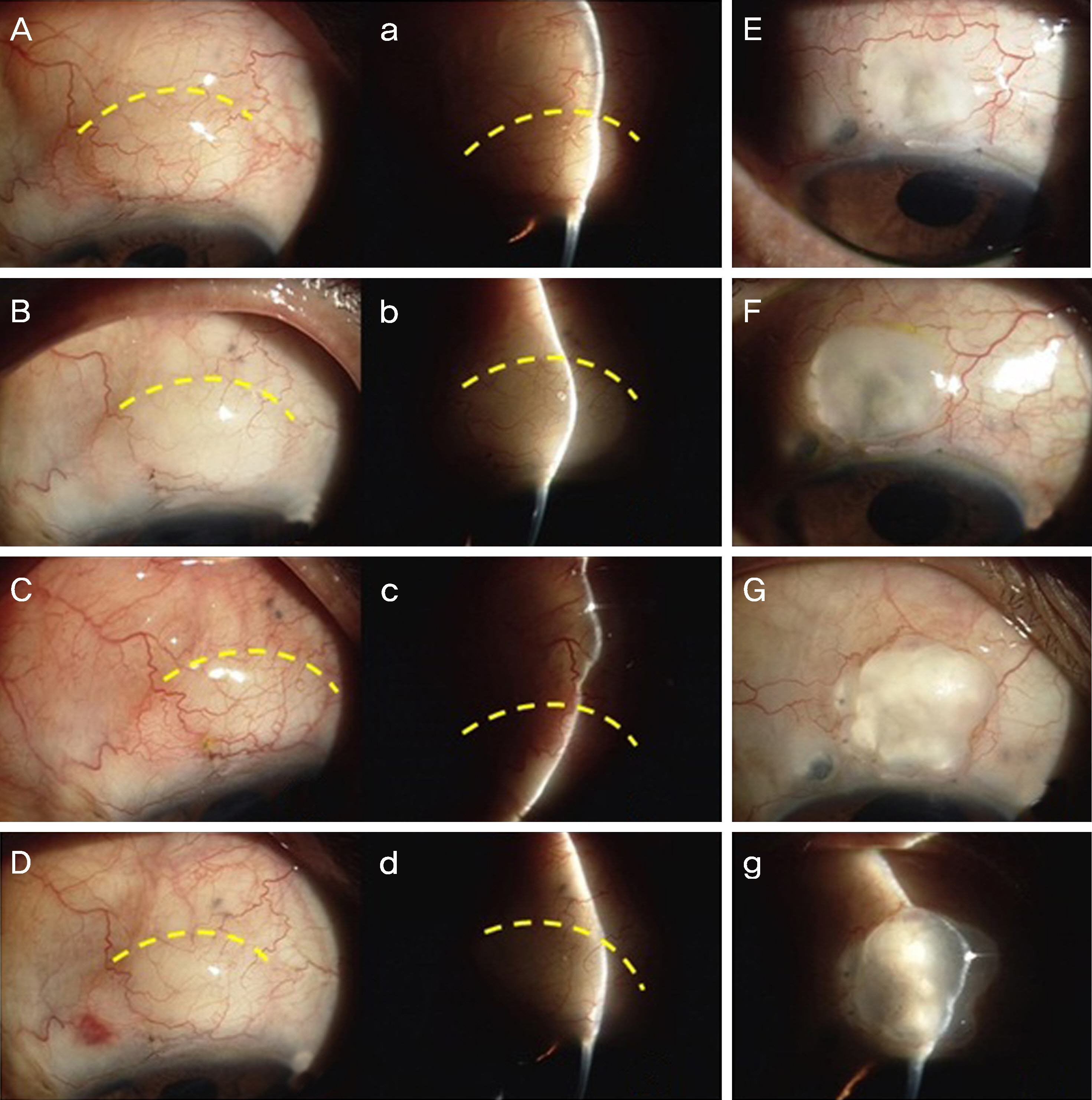
Figure 4. Anterior segment photographs of a 65-year-old male who had trabeculectomy with Ologen® insertion on left eye (A-D, a-d) and conventional trabeculectomy on right eye (E-G, g) due to primary open-angle glaucoma. The dotted yellow curved line is the posterior boundary of the Ologen®. (A, a) At postoperative 1 month, there was mild conjunctival hyperemia and a posterior, diffusely elevated bleb. The intraocular pressure (IOP) was 9 mmHg. (B, b) At postoperative 2 months, an encapsulated bleb without posterior bleb elevation was observed, with an IOP of 30 mmHg. Needling with subconjunctival 5-fluorouracil injection was performed. (C, c) One week after needling, conjunctival hyperemia and a posterior highly elevated bleb were observed. The IOP was 9 mmHg. (D, d) At postoperative 10 months, some conjunctival hyperemia and a posterior, mildly elevated bleb were observed. The IOP was 17 mmHg. (E) At postoperative 3 months, the IOP was 10 mmHg. (F) At postoperative 6 months, the IOP was 16 mmHg. (G, g) At postoperative 12 months, the IOP was 12 mmHg. The right eye showed avascular bleb.
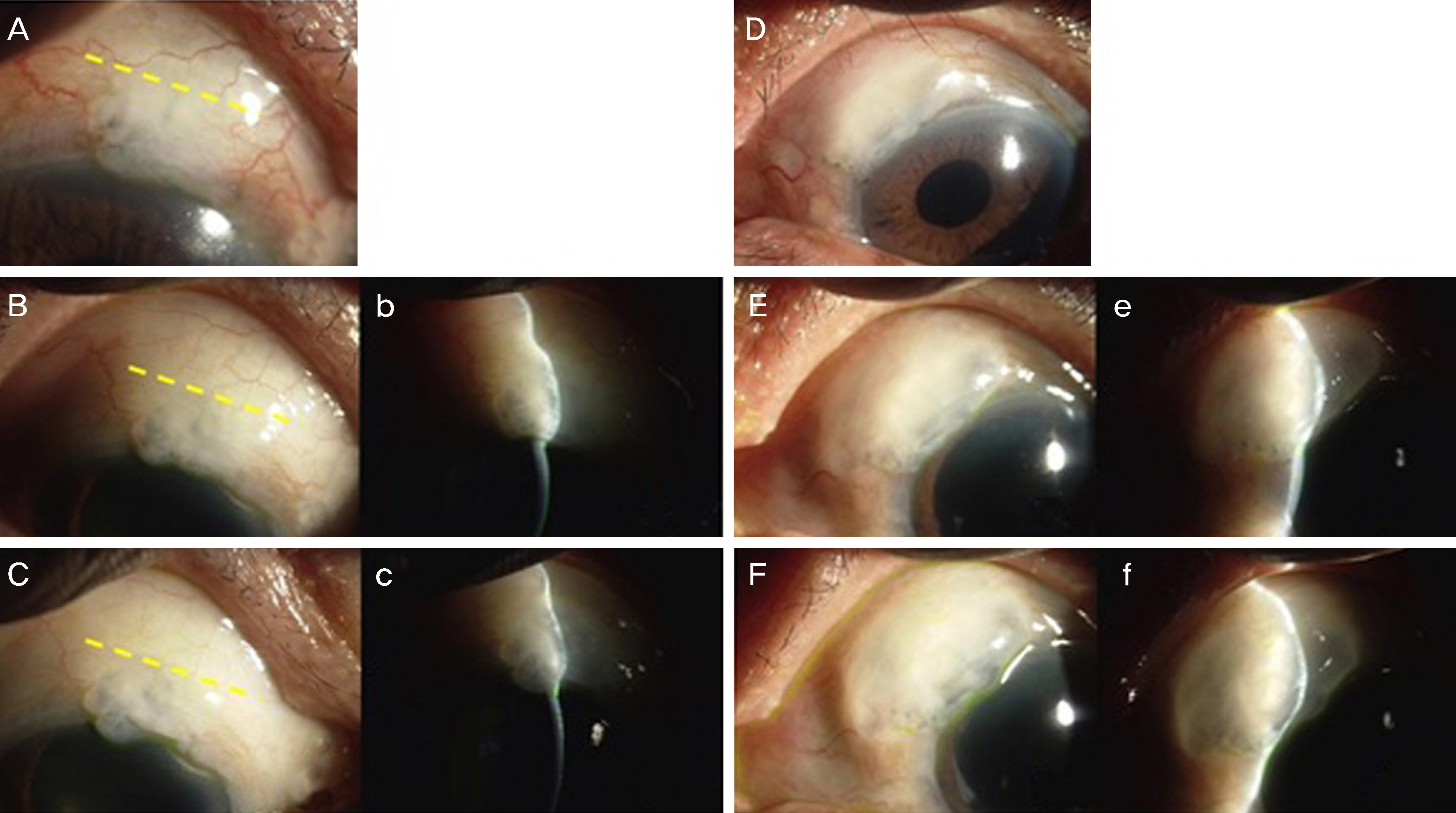
Figure 5. Anterior segment photograghs of a 67-year-old male who had trabeculectomy with Ologen® insertion on right eye (A-C, b, c) and conventional trabeculectomy on left eye (D-F, e, f). The dotted yellow line is the anterior boundary of the Ologen®. (A) At postoperative 2 months, the intraocular pressure (IOP) was 10 mmHg. (B, b) At postoperative 6 months, the IOP was 12 mmHg. (C, c) At postoperative 14 months, the IOP was 10 mmHg. An avascular lesion of the bleb was localized anterior to the Ologen®. A diffuse bleb, which was not avascular, was observed posterior to the avascular lesion. (D) At postoperative 3 months, the IOP was 13 mmHg. (E, e) At postoperative 7 months, the IOP was 11 mmHg. (F, f) At postoperative 15 months, the IOP was 13 mmHg. A wide diffuse avascular bleb was observed.
Reference
-
References
1. Cairns JE. Trabeculectomy. Preliminary report of a new method. Am J Ophthalmol. 1968; 66:673–9.2. Sugar HS. Experimental trabeculectomy in glaucoma. Am J Ophthalmol. 1961; 51:623–7.
Article3. Cheng JW, Xi GL, Wei RL, et al. Efficacy and tolerability of non-penetrating glaucoma surgery augmented with mitomycin C in treatment of open-angle glaucoma: a meta-analysis. Can J Ophthalmol. 2009; 44:76–82.
Article4. Palanca-Capistrano AM, Hall J, Cantor LB, et al. abdominal abdominals of intraoperative 5-fluorouracil versus intraoperative abdominal C in primary trabeculectomy surgery. Ophthalmology. 2009; 116:185–90.5. Anand N, Arora S, Clowes M. Mitomycin C augmented glaucoma surgery: evolution of filtering bleb avascularity, transconjunctival oozing, and leaks. Br J Ophthalmol. 2006; 90:175–80.
Article6. Cillino S, Casuccio A, Di Pace F, et al. Biodegradable collagen abdominal implant versus mitomycin-C in trabeculectomy: five-year fol-low-up. BMC Ophthalmol. 2016; 16:24.
Article7. Cillino S, Di Pace F, Cillino G, Casuccio A. Biodegradable abdominal matrix implant vs mitomycin-C as an adjuvant in abdominal: a 24-month, randomized clinical trial. Eye (Lond). 2011; 25:1598–606.8. Angmo D, Wadhwani M, Upadhyay AD, et al. Outcomes of abdominal augmented with subconjunctival and subscleral ologen implantation in primary advanced glaucoma. J Glaucoma. 2017; 26:8–14.9. Dada T, Kusumesh R, Bali SJ, et al. Trabeculectomy with abdominal use of subconjunctival collagen implant and low-dose abdominal C. J Glaucoma. 2013; 22:659–62.10. Chen HS, Ritch R, Krupin T, Hsu WC. Control of filtering bleb structure through tissue bioengineering: An animal model. Invest Ophthalmol Vis Sci. 2006; 47:5310–4.
Article11. Hsu WC, Ritch R, Krupin T, Chen HS. Tissue bioengineering for surgical bleb defects: an animal study. Graefes Arch Clin Exp Ophthalmol. 2008; 246:709–17.
Article12. Hsu WC, Spilker MH, Yannas IV, Rubin PA. Inhibition of abdominal scarring and contraction by a porous collagen-abdominal implant. Invest Ophthalmol Vis Sci. 2000; 41:2404–11.13. Lee SJ, Woo JM, Min JK, et al. The analysis of the clinical findings and effects of biodegradable collagen matrix in trabeculectomy. J Korean Ophthalmol Soc. 2012; 53:297–305.
Article14. Azura-Blanco A, Katz LJ. Dysfunctional filtering blebs. Surv Ophthalmol. 1998; 43:93–126.15. Mietz H, Arnold G, Kirchhof B, et al. Histopathology of episcrelal fibrosis after trabeculectomy with and without mitomycin C. Graefes Arch Clin Exp Ophthalmol. 1996; 234:364–8.16. Palmer SS. Mitomycin as adjunct chemotherapy with abdominal. Ophthalmology. 1991; 98:317–21.17. Chen CW. Enhanced intraocular pressure controlling effectiveness of trabeculectomy by local application of mitomycin C. Trans Asia Pac Acad Ophthalmol. 1983; 9:172–7.18. Flourouracil Filtering Surgery Study Group. Flourouracil Filtering Surgery Study one-year follow up. Am J Ophthalmol. 1989; 108:625–35.19. Khaw PT, Sherwood MB, Doyle JW, et al. Intraoperative and abdominal treatment with 5-flourouracil and mitomycin-c: long term effects in vivo on subconjunctival and scleral fibroblast. Int Ophthalmol. 1992; 16:381–5.20. Wohlhueter RM, McIvor RS, Plagemann PG. Facilitated transport of uracil and 5-fluorouracil, and permeation of orotic acid into abdominal mammalian cells. J Cell Physiol. 1980; 104:309–19.21. Lockwood A, Brocchini S, Khaw PT. New developments in the pharmacological modulation of wound healing after glaucoma abdominal surgery. Curr Opin Pharmacol. 2013; 13:65–71.22. Rennekampff HO, Hansbrough JF, Kiessig V, et al. Bioactive inter-leukin-8 is expressed in wounds and enhances wound healing. J Surg Res. 2000; 93:41–54.
Article23. Chou SF, Chang SW, Chuang JL. Mitomycin C upregulates IL-8 and MCP-1chemokine expression via mitogen-activated protein kinases in corneal fibroblasts. Invest Ophthalmol Vis Sci. 2007; 48:2009–16.24. Bindlish R, Condon GP, Schlosser JD, et al. Efficacy and safety of mitomycin-C in primary trabeculectomy: five-year follow-up. Ophthalmology. 2002; 109:1336–41. discussion 1341–2.25. Busbee BG, Recchia FM, Kaiser R, et al. Bleb-associated endophthalmitis: clinical characteristics and visual outcomes. abdominalogy. 2004; 111:1495–503. discussion 1503.26. Sapitro J, Dunmire JJ, Scott SE, et al. Suppression of transforming growth factor-β effects in rabbit subconjunctival fibroblasts by ac-tivin receptor-like kinase 5 inhibitor. Mol Vis. 2010; 16:1880–92.27. Na JH, Sung KR, Shin JA, Moon JI. Antifibrotic effects of pirfeni-done on Tenon's fibroblasts in glaucomatous eyes: comparison with mitomycin C and 5-fluorouracil. Graefes Arch Clin Exp Ophthalmol. 2015; 253:1537–45.
Article28. Van Bergen T, Vandewalle E, Moons L, Stalmans I. abdominal effects of bevacizumab and MMC in the improvement of abdominal outcome after glaucoma filtration surgery. Acta Ophthalmol. 2015; 93:667–78.29. Schoenberg ED, Blake DA, Swann FB, et al. Effect of two novel sustained-release drug delivery systems on bleb fibrosis: An in vivo glaucoma drainage device study in a rabbit model. Transl Vis Sci Technol. 2015; 4:4. eCollection 2015 May.
Article30. Min JK, Kee CW, Sohn SW, et al. Surgical outcome of mitomycin C-soaked collagen matrix implant in trabeculectomy. J Glaucoma. 2013; 6:456–62.
Article31. Lama PJ, Fechtner RD. Antifibrotics and wound healing in abdominal surgery. Surv Ophthalmol. 2003; 48:314–46.32. Castner DG, Ratner BD. Biomedical surface science: Foundations to frontiers. Surface Science. 2002; 500:28–60.
Article33. Hong S, Lee JR, Choi JY, et al. Trabeculectomy with biodegradable collagen material: A report of two cases. J Korean Ophthalmol Soc. 2010; 51:912–8.
Article34. Hong S, Lee JR, Kim YD, et al. Fibrous encapsulation of abdominal collagen matrix after trabeculectomy: A case report. J Korean Ophthalmol Soc. 2010; 51:631–5.35. Broadway DC, Bloom PA, Bunce C, et al. Needle revision of failing and failed trabeculectomy blebs with adjunctive5-fluorouracil. Am J Ophthalmol. 2004; 111:665–73.36. Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012; 153:804–14.e1.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fibrous Encapsulation of Biodegradable Collagen Matrix After Trabeculectomy: A Case Report
- The Analysis of the Clinical Findings and Effects of Biodegradable Collagen Matrix in Trabeculectomy
- A Clinical Evaluations of Trabeculectomy
- Surgical Outcomes of Conventional Trabeculectomy Converted from Deep Sclerectomy with Collagen Implant (DSCI)
- Neovascular Glaucoma with Diabetic Retinopathy: Trabeculectomy and Nd:YAG Cyclophotocoagulation
