Primary Pulmonary Extranodal Natural Killer/T-cell Lymphoma, Nasal Type Presenting as Diffuse Ground Glass Opacities: a Case Report
- Affiliations
-
- 1Division of Pulmonology, Department of Internal Medicine, Severance Hospital, Institute of Chest Diseases, Yonsei University College of Medicine, Seoul, Korea. dobie@yuhs.ac
- 2Department of Pathology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 3Division of Hematology, Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2400450
- DOI: http://doi.org/10.3346/jkms.2017.32.10.1727
Abstract
- Extranodal natural killer (NK)/T-cell lymphoma, nasal type (ENKTCL) is a rare type of lymphoma that accounts for only 5%-18% of all cases of non-Hodgkin lymphoma (NHL). In published series, 60%-90% of NK/T-cell lymphomas are localized to the nasal and upper airway. We describe a 55-year man who presented with cough, sputum, dyspnea on exertion, and a chest computed tomography scan shows diffuse ground glass opacities (GGOs), suggestive of an interstitial lung disease. He was treated with a corticosteroid and his symptoms improved. However, when the corticosteroid was tapered, his symptoms recurred. The patient underwent a surgical lung biopsy and ENKTCL was diagnosed. We present this case because ENKTCL involving only the lung is very rare but very informative. To our knowledge, our patient is the first case that primary pulmonary ENKTCL is presented with GGOs.
Keyword
MeSH Terms
Figure
-
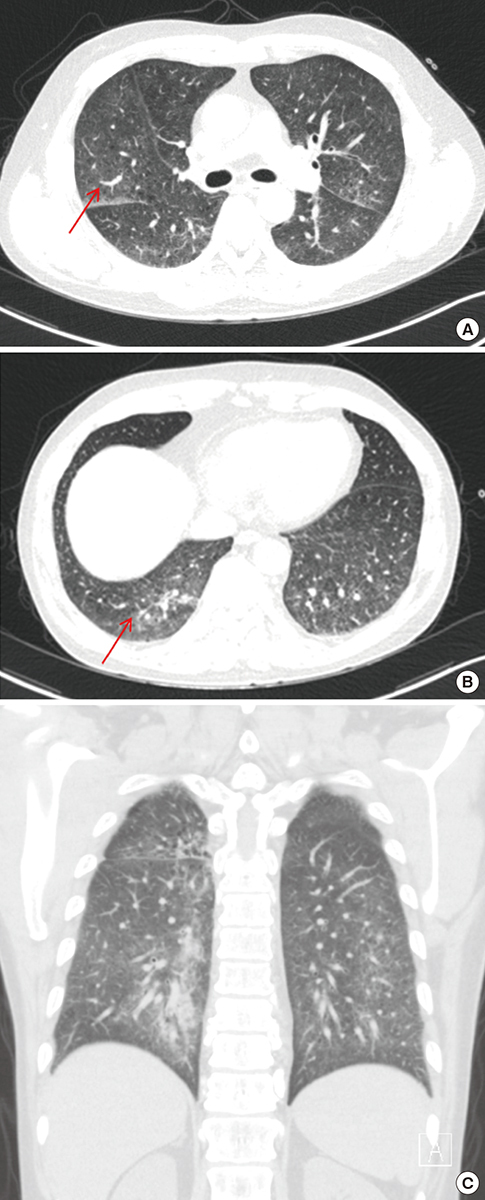
Fig. 1 Follow-up CT scan shows diffuse GGOs at both lungs with underlying emphysema. Arrows indicate sites of wedge resections. Posterior basal segment of right lower lobe (A) and lateral segment of right middle lobe (B). (A, B) Axial view. (C) Coronal view. CT = computed tomography, GGOs = ground glass opacities.
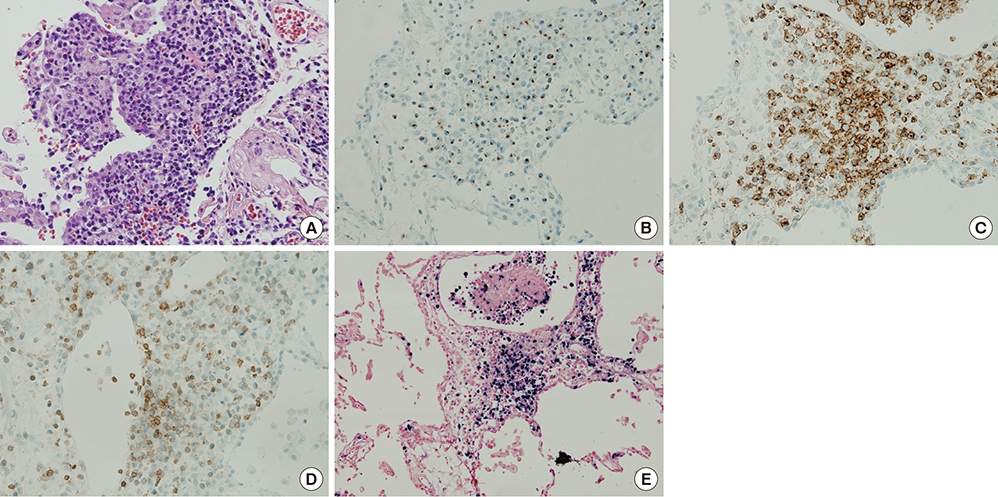
Fig. 2 Histopathology of the lung biopsy. (A) Angiocentric infiltration of the lung parenchyme (magnification × 200). (B) Neoplastic cells stained for granzyme B (magnification × 200). (C) Neoplastic cells stained for CD2 (magnification × 200). (D) Neoplastic cells with loss of expression for surface CD3 (magnification × 200). (E) EBERs by in situ hybridization (magnification × 100). EBERs = Epstein-Barr virus encoded small nuclear RNAs.
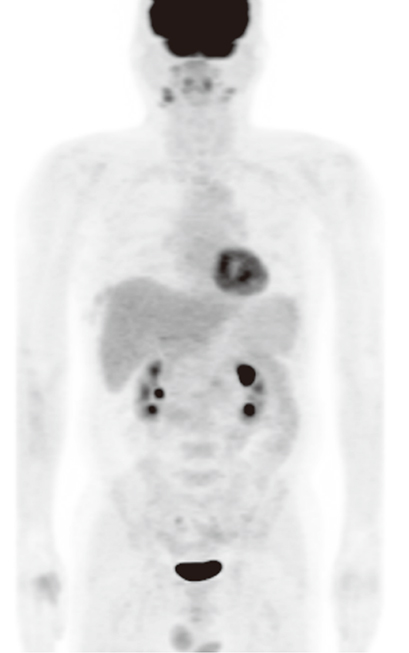
Fig. 3 PET-CT scan shows no significant FDG uptake to suggest malignancy. The lung where ENKTCL is confirmed by biopsy also shows no FDG uptake. PET-CT = positron emission tomography-computed tomography, FDG = fluorodeoxyglucose, ENKTCL = extranodal natural killer/T-cell lymphoma, nasal type.
Reference
-
1. Laohaburanakit P, Hardin KA. NK/T cell lymphoma of the lung: a case report and review of literature. Thorax. 2006; 61:267–270.2. Morovic A, Aurer I, Dotlic S, Weisenburger DD, Nola M. NK cell lymphoma, nasal type, with massive lung involvement: a case report. J Hematop. 2010; 3:19–22.3. Al-Hakeem DA, Fedele S, Carlos R, Porter S. Extranodal NK/T-cell lymphoma, nasal type. Oral Oncol. 2007; 43:4–14.4. Tse E, Liang RH. Natural killer cell neoplasms. Clin Lymphoma. 2004; 5:197–201.5. Kanavaros P, Lescs MC, Brière J, Divine M, Galateau F, Joab I, Bosq J, Farcet JP, Reyes F, Gaulard P. Nasal T-cell lymphoma: a clinicopathologic entity associated with peculiar phenotype and with Epstein-Barr virus. Blood. 1993; 81:2688–2695.6. Chim CS, Ma SY, Au WY, Choy C, Lie AK, Liang R, Yau CC, Kwong YL. Primary nasal natural killer cell lymphoma: long-term treatment outcome and relationship with the International Prognostic Index. Blood. 2004; 103:216–221.7. Suzuki R, Takeuchi K, Ohshima K, Nakamura S. Extranodal NK/T-cell lymphoma: diagnosis and treatment cues. Hematol Oncol. 2008; 26:66–72.8. Aozasa K, Takakuwa T, Hongyo T, Yang WI. Nasal NK/T-cell lymphoma: epidemiology and pathogenesis. Int J Hematol. 2008; 87:110–117.9. Cheung MM, Chan JK, Wong KF. Natural killer cell neoplasms: a distinctive group of highly aggressive lymphomas/leukemias. Semin Hematol. 2003; 40:221–232.10. Lee J, Kim WS, Park YH, Park SH, Park KW, Kang JH, Lee SS, Lee SI, Lee SH, Kim K, et al. Nasal-type NK/T cell lymphoma: clinical features and treatment outcome. Br J Cancer. 2005; 92:1226–1230.11. Lee BH, Kim SY, Kim MY, Hwang YJ, Han YH, Seo JW, Kim YH, Cha SJ, Hur G. CT of nasal-type T/NK cell lymphoma in the lung. J Thorac Imaging. 2006; 21:37–39.12. Oshima K, Tanino Y, Sato S, Inokoshi Y, Saito J, Ishida T, Fukuda T, Watanabe K, Munakata M. Primary pulmonary extranodal natural killer/T-cell lymphoma: nasal type with multiple nodules. Eur Respir J. 2012; 40:795–798.13. Fei W, Xiaohong W, Hong Z, Bei H. Pulmonary extranodal natural killer/T-cell lymphoma (nasal type): a case report and radiological image review. Medicine (Baltimore). 2015; 94:e1527.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Metachronous extranodal natural killer/T-cell lymphoma of nasal type and primary testicular lymphoma
- Extranodal NK/T-Cell Lymphoma, Nasal Type, Extranasal and Ulcerative Blister Variant, Case Report
- Delayed Diagnosis Due to Septal Perforation in Patient with Extranodal Natural Killer/T-Cell Lymphoma, Nasal Type
- A Case of Extranodal Natural Killer/T Cell Lymphoma Combined With Actinomycosis
- A Case of Extranodal NK/T-cell Lymphoma at the Base of Tongue
