Surgical Reconstruction of Nasal Alar Deformities
- Affiliations
-
- 1Department of Dermatology, School of Medicine, Chosun University, Gwangju, Korea.
- 2Department of Otorhinolaryngology-Head and Neck Surgery, School of Medicine, Chosun University, Gwangju, Korea. happyent@naver.com
- KMID: 2398823
- DOI: http://doi.org/10.18787/jr.2017.24.2.65
Abstract
- Reconstruction of the nasal alar may be challenging due to the complex nature of multiple cosmetic units and functional considerations, including maintenance of valvular competency. Reconstructive options include various flaps or graft repairs, depending on the subunit involvement and the size of the defect. Linear closures may be suitable for small defects, while bilobed flaps, melolabial flaps, and forehead flaps may be considered for moderate to large defects involving partial and full-thickness defects of the ala.
MeSH Terms
Figure
-
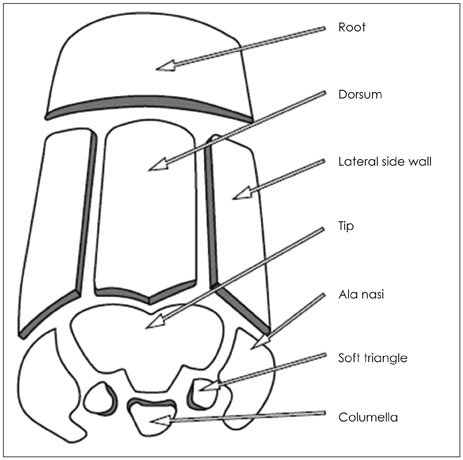
Fig. 1 Nasal aesthetic subunit. The specific topographic subunits that they identified as the dorsum, tip, and columella and the paired alae, sidewalls, and soft triangles.
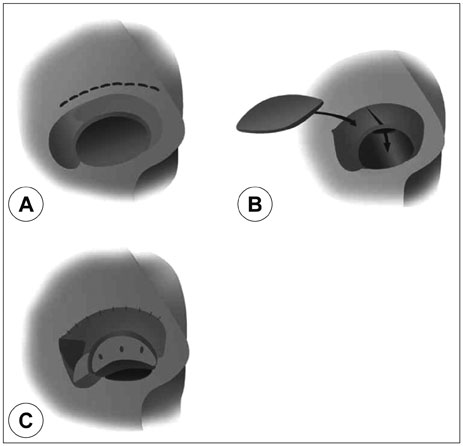
Fig. 2 Bipedicle vestibular skin advancement flap. A: Make intercartilagenous incision between upper and lower lateral cartilages. B: Elevate the flap, sufficiently to mobilize. C: Auricular cartilage can serve as framework.

Fig. 3 Ipsilateral septal mucoperichondrial hinge flap. A: Unipedicle septal mucoperichondrial hinge flap developed by incising through mucosa and perichondrium along floor of nose and 1.5 cm below and parallel to cartilaginous dorsum. Incisions extend posteriorly beyond septal bony cartilaginous junction. B: Flap dissected from superior to inferior and anterior to posterior. Anterior dissection remains 1 cm posterior to caudal border of septum and 1.5 cm posterior to nasal spine. Flap based on intact mucoperichondrium of caudal septum and septal branch of superior labial artery. C: Hinged on caudal septum, flap is reflected laterally to line lower nasal vault. D: Cartilage graft provides nasal framework. Lining flap secured to framework with mattress sutures (From Baker SR: Internal lining. In Baker SR, editor: Principles of nasal reconstruction, ed 2, New York, Springer, 2011).
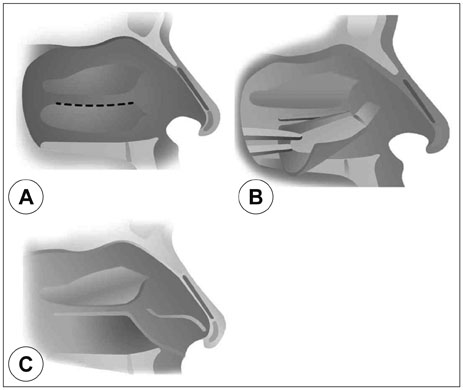
Fig. 4 Turbinate mucoperiosteal flap. A: Turbinate flap is released from posterior to anterior with a periosteal elevator. The anterior pedicle is left intact. B: The posterior turbinate is grasped with a Takahashi forceps and delivered through the defect or nostril. C: The conchal bone is removed as the turbinate is bivalved open. The flap is sutured into position and the nose is packed with a light sponge pack.

Fig. 5 Skin graft. A: Middle aged man was squamous cell cancer on right alar area. B: The lesion was removed and covered by skin graft from preauricular area. C: 2 months after operation show well healed state.
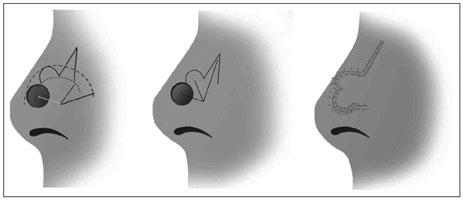
Fig. 6 Bilobed flap. Orientation of the standard Zitelli bilobed flap design on the nasal sidewall.
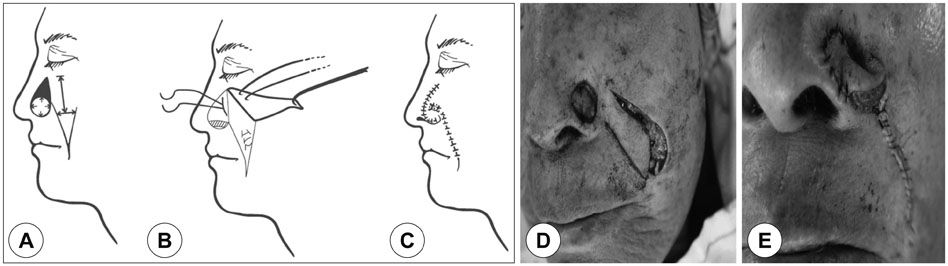
Fig. 7 Superiorly based single-staged melolabial flap. A: Lateral nasal skin (shaded) is excised to the nasofacial border to facilitate flap insertion. B: Flap incision and lateral retraction allows plication of the superficial musculoaponeurotic system. Rim-stabilizing cartilage graft prevents alar retraction. Nasojugal crease reconstruction is secured by permanent sutures anchoring the flap to the periosteum. C: The resultant suture line is camouflaged by the melolabial crease. D and E: Intraoperative photos of superiorly based melolabila flap.

Fig. 8 Two-staged melolabial interpolation flap repair. Design and correction of alar skin defect using melolabial flap.
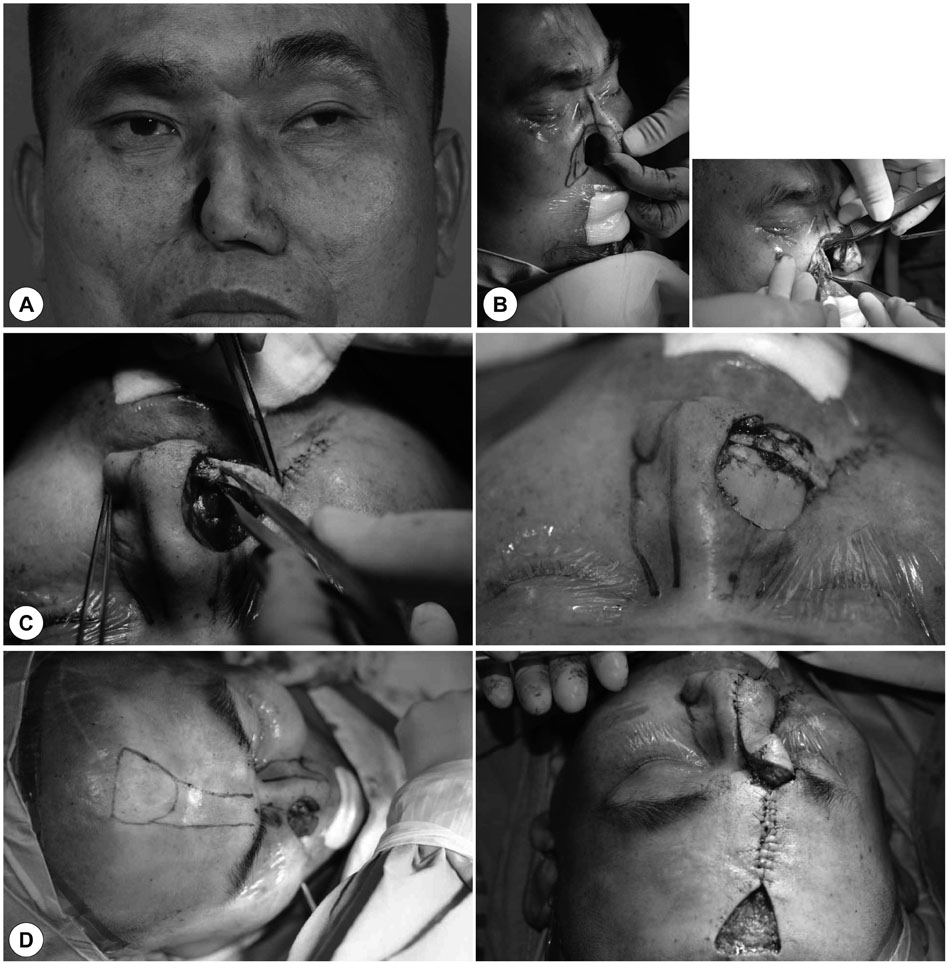
Fig. 9 Forehead flap. A: 45 years old man shows dorsal and alar defect developed after resection and radiation therapy of malignant melanoma of nasal cavity. B: For internal lining of external nose, design a turn in flap from nasal dorsum and cheek skin. C: For structural frame work, reconstruction of upper and lower lateral cartilage using autologous costal cartilage. D: Skin defect was covered by forehead flap.
Reference
-
1. David AS, Wayne FL. Principles of facial reconstruction. New York: Thieme;2009. p. 102–160.2. Burget GC, Menick FJ. Aesthetic Reconstruction of the Nose. St Louis, MO: Mosby Year Book Inc;1993.3. Driscoll BP, Baker SR. Reconstruction of nasal alar defects. Arch Facial Plast Surg. 2001; 3(2):91–99.
Article4. Byrd DR, Otley CC, Nguyen TH. Alar batten cartilage grafting in nasal reconstruction: functional and cosmetic results. J Am Acad Dermatol. 2000; 43(5 Pt 1):833–836.
Article5. Woodard CR, Park SS. Reconstruction of nasal defects 1.5 cm or smaller. Arch Facial Plast Surg. 2011; 13(2):97–102.
Article6. Murakami CS, Kriet D, Ierokomos AP. Nasal reconstruction using the inferior turbinate mucosal flap. Arch Facial Plast Surg. 1999; 1:97–100.
Article7. Barlow JO. The placement of structural cartilage grafts under full-thickness skin grafts: a case series and strategies for successful outcomes. Dermatol Surg. 2010; 36(7):1166–1170.
Article8. Adams DC, Ramsey ML. Grafts in dermatologic surgery: review and update on full- and split-thickness skin grafts, free cartilage grafts, and composite grafts. Dermatol Surg. 2005; 31(8 Pt 2):1055–1067.
Article9. Shaye DA, Jonathan MS, Kim JE. Advances in nasal reconstruction. Curr Opin Otolaryngol Head Neck Surg. 2011; 19:251–256.
Article10. Zitelli JA, Fazio MJ. Reconstruction of the nose with local flaps. J Dermatol Surg Oncol. 1991; 17(2):184–189.
Article11. Lindsey WH. Reliability of the melolabial flap for alar reconstruction. Arch Facial Plast Surg. 2001; 3(1):33–37.
Article12. Zitelli JA. The nasolabial flap as a single-stage procedure. Arch Dermatol. 1990; 126(11):1445–1448.
Article13. Baker SR. Local flaps in facial reconstruction. 2nd edition. St. Louis: Mosby;2008. p. 415–474.14. van der Eerden PA, Verdam FJ, Dennis SCR, Vuyk H. Free cartilage grafts and healing by secondary intention: a viable reconstructive combination after excision of nonmelanoma skin cancer in the nasal alar region. Arch Facial Plast Surg. 2009; 11(1):18–23.15. Baker SR, Johnston TM, Nelson BR. The importance of maintaining the alar-facial sulcus in nasal reconstruction. Arch Otolaryngol Head Neck Surg. 1995; 121:617–622.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Novel Approach for Full-Thickness Defect of the Nasal Alar Rim: Primary Closure of the Defect and Reduction of the Contralateral Normal Ala for Symmetry
- Diagnosis and Treatment of Alar Rim Deformities
- Reconstruction of Postburn Nasal Alar Defect by Paramedian Forehead Flap
- Alar Base Augmentation by Various Methods in Secondary Lip Nasal Deformity
- A case of alar stenosis: single-staged alar reconstruction
